The twenty-first century role of Piver-Rutledge type III radical hysterectomy and FIGO stage IA, IB1, and IB2 cervical cancer in the era of robotic surgery: a personal perspective
- Affiliations
-
- 1Department of Gynecology, Sisters of Charity Hospital, Buffalo, NY, USA. mpiver@chsbuffalo.org
- KMID: 2173544
- DOI: http://doi.org/10.3802/jgo.2010.21.4.219
Abstract
- Type III radical hysterectomy reported in 1974 by Piver, Rutledge, and Smith is considered worldwide by many as the standard surgical therapy for invasive cervical carcinoma stage IB and IIA. With the increasing number of robotic surgeries being performed for early stage cervical cancer worldwide, the purpose of the paper is to present our personal perspective of the 21st century role of Piver-Rutledge type III radical hysterectomy for stage IB cervical cancer in the era of robotic surgery using the da Vinci robot.
MeSH Terms
Figure
-
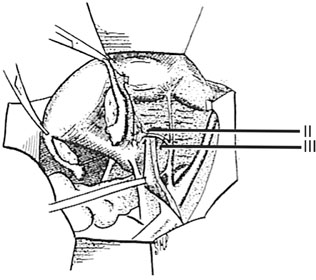
Fig. 1 In a class II hysterectomy the uterine artery is ligated medical to the ureter, whereas in a class III it is ligated as it originates from the internal iliac artery. From Piver MS, et al. Obstet Gynecol 1974; 44: 265-72, with permission from Obstetrics & Gynecology.5

Fig. 2 In a class II hysterectomy the uterosacral ligaments are divided midway between the uterus and their sacral attachments. In a class III operation the uterosacral ligaments are excised at their sacral attachments. From Piver MS, et al. Obstet Gynecol 1974; 44: 265-72, with permission from Obstetrics & Gynecology.5
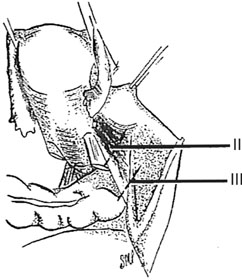
Fig. 3 The medial one-half of the cardinal ligament is removed in a class II hysterectomy. In a class III operation the cardinal ligament is removed at the pelvic wall. From Piver MS, et al. Obstet Gynecol 1974; 44: 265-72, with permission from Obstetrics & Gynecology.5
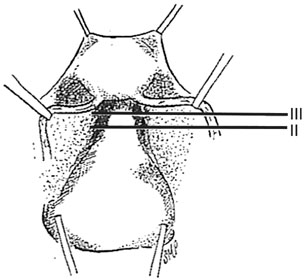
Fig. 4 The upper one-third of the vagina is removed in a class II hysterectomy and one-half in a class III procedure. Not illustrated is removal of three-fourths of the vagina in class IV hysterectomy. From Piver MS, et al. Obstet Gynecol 1974; 44: 265-72, with permission from Obstetrics & Gynecology.5
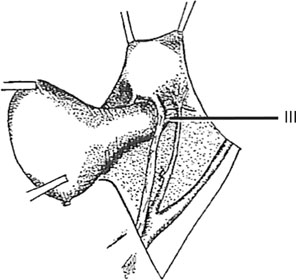
Fig. 5 In a class III hysterectomy the ureter is dissected from the pubovesicle ligament superiorly, medially, and inferiorly. A small lateral portion of the pubovesicle artery is preserved, thus maintaining some blood supply to the distal ureter. From Piver MS, et al. Obstet Gynecol 1974; 44: 265-72, with permission from Obstetrics & Gynecology.5
Reference
-
1. Moore DH. Cervical cancer. Obstet Gynecol. 2006. 107:1152–1161.2. Pecorelli S, Zigliani L, Odicino F. Revised FIGO staging for carcinoma of the cervix. Int J Gynaecol Obstet. 2009. 105:107–108.3. Piver MS, Lee JY. The 21st century role of Piver type II hysterectomy in FIGO stage IA, IB cervical cancer: a personal perspective. Eur J Gynaecol Oncol. 2008. 29:109–113.4. Piver MS, Chung WS. Prognostic significance of cervical lesion size and pelvic node metastases in cervical carcinoma. Obstet Gynecol. 1975. 46:507–510.5. Piver MS, Rutledge F, Smith JP. Five classes of extended hysterectomy for women with cervical cancer. Obstet Gynecol. 1974. 44:265–272.6. Pikaart DP, Holloway RW, Ahmad S, Finkler NJ, Bigsby GE 4th, Ortiz BH, et al. Clinical-pathologic and morbidity analyses of Types 2 and 3 abdominal radical hysterectomy for cervical cancer. Gynecol Oncol. 2007. 107:205–210.7. Wertheim E. Zur frage der radicaloperation beim uteruskrebs. Arch Gynecol. 1900. 61:627–668.8. Meigs JV. Radical hysterectomy with bilateral pelvic lymph node dissections: a report of 100 patients operated on five or more years ago. Am J Obstet Gynecol. 1951. 62:854–870.9. Querleu D, Leblanc E, Castelain B. Pelvic lymphadenectomy under celioscopic guidance. J Gynecol Obstet Biol Reprod (Paris). 1990. 19:576–578.10. Nezhat CR, Burrell MO, Nezhat FR, Benigno BB, Welander CE. Laparoscopic radical hysterectomy with paraaortic and pelvic node dissection. Am J Obstet Gynecol. 1992. 166:864–865.11. Magrina JF. Robotic surgery in gynecology. Eur J Gynaecol Oncol. 2007. 28:77–82.12. Zakashansky K, Bradley WH, Nezhat FR. New techniques in radical hysterectomy. Curr Opin Obstet Gynecol. 2008. 20:14–19.13. Zakashansky K, Bradley WH, Chuang L, Rahaman J, Dottino P. Recent advances in the surgical management of cervical cancer. Mt Sinai J Med. 2009. 76:567–576.14. Ercoli A, Iannone V, Legge F, Fagotti A, Fanfani F, Carone V, et al. Advances in surgical management of cervical cancer. Minerva Ginecol. 2009. 61:227–237.15. Ramirez PT. Robotic radical hysterectomy: a new standard of care? Future Oncol. 2009. 5:23–25.16. Fanning J, Hojat R, Johnson J, Fenton B. Robotic radical hysterectomy. Minerva Ginecol. 2009. 61:53–55.17. Magrina JF, Kho R, Magtibay PM. Robotic radical hysterectomy: technical aspects. Gynecol Oncol. 2009. 113:28–31.18. Bandera CA, Magrina JF. Robotic surgery in gynecologic oncology. Curr Opin Obstet Gynecol. 2009. 21:25–30.19. Magrina JF, Zanagnolo VL. Robotic surgery for cervical cancer. Yonsei Med J. 2008. 49:879–885.20. Sert BM, Abeler VM. Robotic-assisted laparoscopic radical hysterectomy (Piver type III) with pelvic node dissection: case report. Eur J Gynaecol Oncol. 2006. 27:531–533.21. Sert B, Abeler V. Robotic radical hysterectomy in early-stage cervical carcinoma patients, comparing results with total laparoscopic radical hysterectomy cases. The future is now? Int J Med Robot. 2007. 3:224–228.22. Kim YT, Kim SW, Hyung WJ, Lee SJ, Nam EJ, Lee WJ. Robotic radical hysterectomy with pelvic lymphadenectomy for cervical carcinoma: a pilot study. Gynecol Oncol. 2008. 108:312–316.23. Magrina JF, Kho RM, Weaver AL, Montero RP, Magtibay PM. Robotic radical hysterectomy: comparison with laparoscopy and laparotomy. Gynecol Oncol. 2008. 109:86–91.24. Fanning J, Fenton B, Purohit M. Robotic radical hysterectomy. Am J Obstet Gynecol. 2008. 198:649.e1–649.e4.25. Nezhat FR, Datta MS, Liu C, Chuang L, Zakashansky K. Robotic radical hysterectomy versus total laparoscopic radical hysterectomy with pelvic lymphadenectomy for treatment of early cervical cancer. JSLS. 2008. 12:227–237.26. Boggess JF, Gehrig PA, Cantrell L, Shafer A, Ridgway M, Skinner EN, et al. A case-control study of robot-assisted type III radical hysterectomy with pelvic lymph node dissection compared with open radical hysterectomy. Am J Obstet Gynecol. 2008. 199:357.e1–357.e7.27. Geisler JP, Orr CJ, Khurshid N, Phibbs G, Manahan KJ. Robotically assisted laparoscopic radical hysterectomy compared with open radical hysterectomy. Int J Gynecol Cancer. 2010. 20:438–442.28. Piver MS, Marchetti DL, Patton T, Halpern J, Blumenson L, Driscoll DL. Radical hysterectomy and pelvic lymphadenectomy versus radiation therapy for small (less than or equal to 3 cm) stage IB cervical carcinoma. Am J Clin Oncol. 1988. 11:21–24.29. Hopkins MP, Morley GW. Radical hysterectomy versus radiation therapy for stage IB squamous cell cancer of the cervix. Cancer. 1991. 68:272–277.30. Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997. 350:535–540.31. Cantrell LA, Mendivil A, Gehrig PA, Boggess JF. Survival outcomes for women undergoing type III robotic radical hysterectomy for cervical cancer: a 3-year experience. Gynecol Oncol. 2010. 117:260–265.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Management of FIGO stage IB2 Cervical Cancer
- A comparison of robot assisted and abdominal radical hysterectomy (RH) for early stage cervical and endometrial cancer
- Comparative study of neoadjuvant chemotherapy before radical hysterectomy and radical surgery alone in stage IB2-IIA bulky cervical cancer
- Clinical Analysis of The Invasive Cervical Cancer Patients Treated by Radical Hysterectomy
- Comparison of laparoscopic and abdominal radical hysterectomy for patients with FIGO stage IB1 cervical cancer
