Ann Surg Treat Res.
2016 Jan;90(1):1-9. 10.4174/astr.2016.90.1.1.
Biologic subtype is a more important prognostic factor than nodal involvement in patients with stages I and II breast carcinoma
- Affiliations
-
- 1Department of Surgery, Keimyung University School of Medicine, Daegu, Korea. shkang9002@gmail.com
- 2Department of Pathology, Keimyung University School of Medicine, Daegu, Korea.
- KMID: 2149925
- DOI: http://doi.org/10.4174/astr.2016.90.1.1
Abstract
- PURPOSE
Nodal infiltration has been one of the most important prognostic factors in breast cancer. In recent decades, risk stratification has greatly changed, and is applied in accordance with hormone receptor and human epidermal growth factor receptor 2 (HER2) status. We compared the prognostic power of tumor subtype to nodal involvement in early breast cancer.
METHODS
We reviewed the medical records of 505 patients who had curative surgery for stage I or II breast cancer. We analyzed clinicopathologic factors according to tumor subtype and nodal involvement. Tumors were classified into 4 subtypes according to immunohistochemical status of estrogen receptor, progesterone receptor, HER2, and Ki67 labeling index. Disease-free survival (DFS) and overall survival were analyzed.
RESULTS
There were 363 node-negative patients (71.9%) and 142 node-positive patients (28.1%). Luminal A, Luminal B, HER2, and triple-negative breast cancer subtypes were composed of 207 (41.0%), 147 (29.1%), 42 (8.3%), and 109 patients (21.6%), respectively. The median follow-up period was 89.5 months. Node negative-luminal A subtype showed the best prognosis with regard to 5-year DFS, and the pN1-triple negative subtype was associated with the shortest DFS (95.1% vs. 67.8%; hazard ratio, 9.554; P < 0.001). However, the node negative-triple negative subtype was associated with a worse 5-year DFS than the pN1-luminal A subtype ([86.4%; hazard ratio, 2.647; P = 0.048] vs. [93.2%; hazard ratio, 2.061; P = 0.194]).
CONCLUSION
Node negative-triple negative breast cancer was associated with a poorer prognosis than pN1-luminal A subtype. Tumor subtype has greater prognostic power compared to nodal status in early breast cancer.
MeSH Terms
-
Breast Neoplasms*
Breast*
Disease-Free Survival
Estrogens
Follow-Up Studies
Humans
Lymphatic Metastasis
Medical Records
Phenobarbital
Prognosis
Receptor, Epidermal Growth Factor
Receptors, Progesterone
Triple Negative Breast Neoplasms
Estrogens
Phenobarbital
Receptor, Epidermal Growth Factor
Receptors, Progesterone
Figure
-
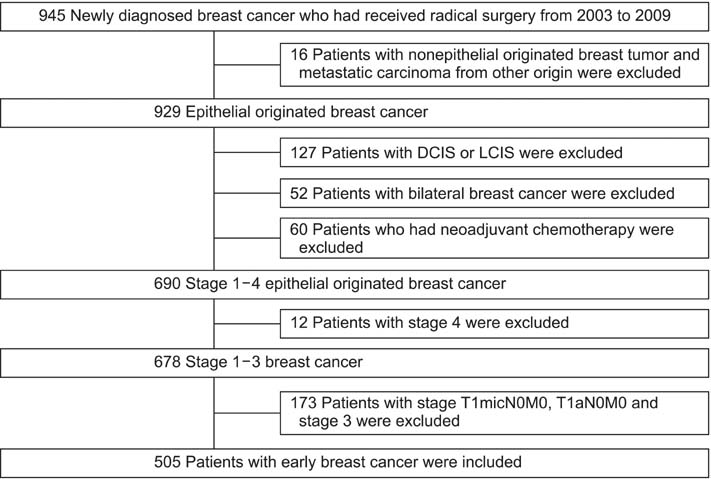
Fig. 1 Description of study population. DCIS, ductal carcinoma in situ; LCIS, lobular carcinoma in situ.
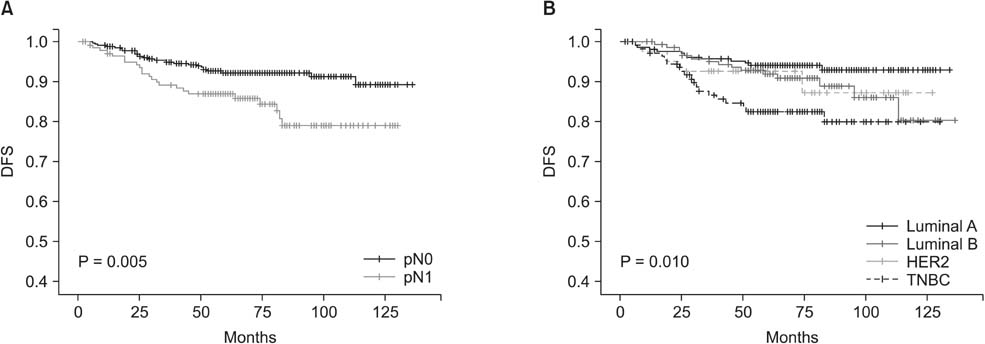
Fig. 2 Disease-free survival (DFS) of total patients according to nodal status (A) and intrinsic subtype (B). HER2, human epidermal growth factor receptor 2; TNBC, triple negative breast cancer.
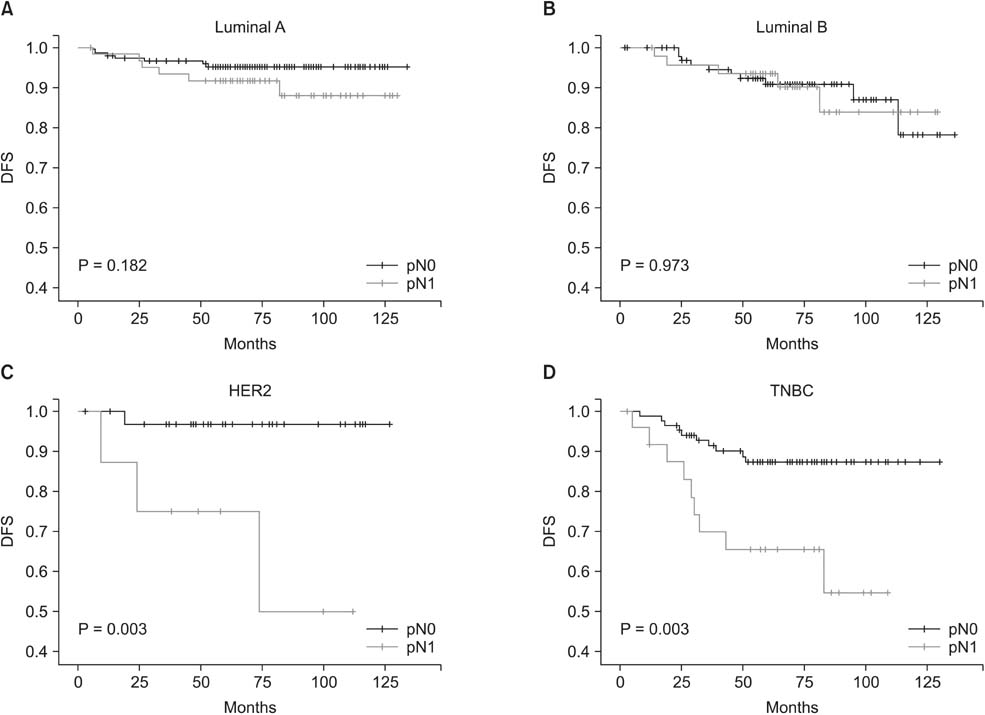
Fig. 3 (A-D) Subgroup analysis of disease-free survival (DFS) according to intrinsic subtype and nodal status. HER2, human epidermal growth factor receptor 2; TNBC, triple negative breast cancer.
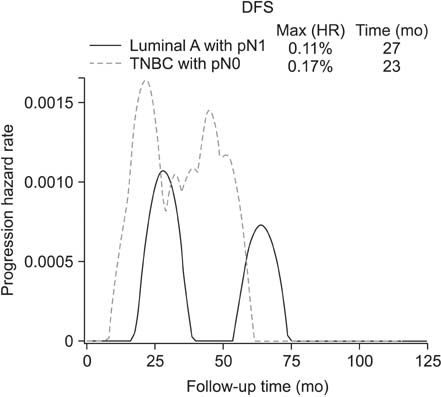
Fig. 4 Progression hazard rate for recurrence between luminal A type with pN1 and triple negative type with pN0. DFS, disease-free survival; TNBC, triple negative breast cancer.
Reference
-
1. Perou CM, Sorlie T, Eisen MB, van de Rijn M, Jeffrey SS, Rees CA, et al. Molecular portraits of human breast tumours. Nature. 2000; 406:747–752.2. Sorlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci U S A. 2001; 98:10869–10874.3. Sorlie T, Tibshirani R, Parker J, Hastie T, Marron JS, Nobel A, et al. Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A. 2003; 100:8418–8423.4. Prat A, Perou CM. Deconstructing the molecular portraits of breast cancer. Mol Oncol. 2011; 5:5–23.5. Goldhirsch A, Winer EP, Coates AS, Gelber RD, Piccart-Gebhart M, Thurlimann B, et al. Personalizing the treatment of women with early breast cancer: highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann Oncol. 2013; 24:2206–2223.6. National Comprehensive Cancer Network. NCCN clinical practice guidelines for treatment of cancer by site: breast cancer [Internet]. Fort Wathington (PA): National Comprehensive Cancer Network;c2015. cited 2015 Feb 5. Available from: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp.7. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010; 17:1471–1474.8. Chia S, Norris B, Speers C, Cheang M, Gilks B, Gown AM, et al. Human epidermal growth factor receptor 2 overexpression as a prognostic factor in a large tissue microarray series of node-negative breast cancers. J Clin Oncol. 2008; 26:5697–5704.9. Park YH, Kim ST, Cho EY, Choi YL, Ok ON, Baek HJ, et al. A risk stratification by hormonal receptors (ER, PgR) and HER-2 status in small (< or = 1 cm) invasive breast cancer: who might be possible candidates for adjuvant treatment? Breast Cancer Res Treat. 2010; 119:653–661.10. Amar S, McCullough AE, Tan W, Geiger XJ, Boughey JC, McNeil RB, et al. Prognosis and outcome of small (<=1 cm), node-negative breast cancer on the basis of hormonal and HER-2 status. Oncologist. 2010; 15:1043–1049.11. Dignam JJ, Dukic V, Anderson SJ, Mamounas EP, Wickerham DL, Wolmark N. Hazard of recurrence and adjuvant treatment effects over time in lymph node-negative breast cancer. Breast Cancer Res Treat. 2009; 116:595–602.12. Liu X, Guan Y, Wang Y, Zhang W, Liu S, Wang L, et al. Relationship between chemotherapy and prognosis in different subtypes of node-negative breast cancer. Tumour Biol. 2014; 35:8581–8589.13. Ribelles N, Perez-Villa L, Jerez JM, Pajares B, Vicioso L, Jimenez B, et al. Pattern of recurrence of early breast cancer is different according to intrinsic subtype and proliferation index. Breast Cancer Res. 2013; 15:R98.14. Chang J, Lee A, Lee J, Lim W, Sung SH, Moon BI. Correlation between the molecular subtype of breast cancer and the in vitro adenosine triphosphate-based chemosensitivity assay. J Korean Surg Soc. 2013; 84:313–320.15. Munzone E, Curigliano G, Burstein HJ, Winer EP, Goldhirsch A. CMF revisited in the 21st century. Ann Oncol. 2012; 23:305–311.16. Cheang M, Chia S, Tu D, Jiang S, Shepherd L, Pritchard K, et al. Anthracyclines in basal breast cancer: the NCIC-CTG trial MA5 comparing adjuvant CMF to CEF. J Clin Oncol. 2009; 27:15 Suppl. Abstract No. 519.17. Colleoni M, Cole BF, Viale G, Regan MM, Price KN, Maiorano E, et al. Classical cyclophosphamide, methotrexate, and fluorouracil chemotherapy is more effective in triple-negative, node-negative breast cancer: results from two randomized trials of adjuvant chemoendocrine therapy for node-negative breast cancer. J Clin Oncol. 2010; 28:2966–2973.18. Rocca A, Bravaccini S, Scarpi E, Mangia A, Petroni S, Puccetti M, et al. Benefit from anthracyclines in relation to biological profiles in early breast cancer. Breast Cancer Res Treat. 2014; 144:307–318.19. Hugh J, Hanson J, Cheang MC, Nielsen TO, Perou CM, Dumontet C, et al. Breast cancer subtypes and response to docetaxel in node-positive breast cancer: use of an immunohistochemical definition in the BCIRG 001 trial. J Clin Oncol. 2009; 27:1168–1176.20. Martín M, Segui MA, Anton A, Ruiz A, Ramos M, Adrover E, et al. Adjuvant docetaxel for high-risk, node-negative breast cancer. N Engl J Med. 2010; 363:2200–2210.21. Jacquin JP, Jones S, Magne N, Chapelle C, Ellis P, Janni W, et al. Docetaxel-containing adjuvant chemotherapy in patients with early stage breast cancer: consistency of effect independent of nodal and biomarker status: a meta-analysis of 14 randomized clinical trials. Breast Cancer Res Treat. 2012; 134:903–913.22. Vaz-Luis I, Ottesen RA, Hughes ME, Mamet R, Burstein HJ, Edge SB, et al. Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: a multi-institutional study. J Clin Oncol. 2014; 32:2142–2150.23. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010; 363:1938–1948.24. Gelmon K, Dent R, Mackey JR, Laing K, McLeod D, Verma S. Targeting triple-negative breast cancer: optimising therapeutic outcomes. Ann Oncol. 2012; 23:2223–2234.25. Yadav BS, Sharma SC, Chanana P, Jhamb S. Systemic treatment strategies for triplenegative breast cancer. World J Clin Oncol. 2014; 5:125–133.26. Abramson VG, Lehmann BD, Ballinger TJ, Pietenpol JA. Subtyping of triple-negative breast cancer: implications for therapy. Cancer. 2015; 121:8–16.27. Joensuu H, Gligorov J. Adjuvant treatments for triple-negative breast cancers. Ann Oncol. 2012; 23:Suppl 6. vi40–vi45.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Breast Cancer Subtype as a Predictor of Lymph Node Metastasis according to the SEER Registry
- Human Epidermal Growth Factor Receptor 2-Subtype Invasive Ductal Carcinoma Recurring as Basal-Human Epidermal Growth Factor Receptor 2-Subtype Squamous Cell Carcinoma
- Metastasis-Free Interval Is Closely Related to Tumor Characteristics and Has Prognostic Value in Breast Cancer Patients with Distant Relapse
- Lymph node metastasis as a prognostic factor in patients with cervical cancer
- Development of an Excel Program for the Updated Eighth American Joint Committee on Cancer Breast Cancer Staging System
