Cardiac Involvement of Churg-Strauss Syndrome as a Reversible Cause of Dilated Cardiomyopathy
- Affiliations
-
- 1Department of Cardiovascular Medicine, Chonnam National University Hospital, Gwangju, Korea. christiankyehun@hanmail.net
- 2Department of Radiology, Chonnam National University Hospital, Gwangju, Korea.
- KMID: 2135406
- DOI: http://doi.org/10.4250/jcu.2015.23.1.40
Abstract
- A 31-year-old male who had been treated for Churg-Strauss syndrome (CSS) presented with sudden onset of dysarthria. Brain magnetic resonance imaging (MRI) showed acute multifocal bilateral cerebral infarctions suggesting embolic causes. Cardiac MRI showed dilated cardiomyopathy with severe biventricular dysfunction with intracardiac thrombi, and multiple high signal intensity spots in myocardium of the left ventricle with multifocal delayed enhancement suggesting multifocal myocarditis due to small vessel vasculitis associated with CSS. After anticoagulation therapy, treatments for heart failure, and immunosuppressive therapy including parenteral steroids and cyclophosphamide to control CSS, the symptoms and signs of heart failure and cardiac function of the patient were improved. Considering the pathophysiologic mechanism of cardiac involvement in CSS, immunosuppressive therapy to control the disease activity of CSS should be taken into account, besides usual management for heart failure.
MeSH Terms
Figure
-

Fig. 1 Magnetic resonance image (MRI) findings of the brain. MRI image findings of the brain reveals multi-focal acute cerebral infarctions (indicated by white arrows).
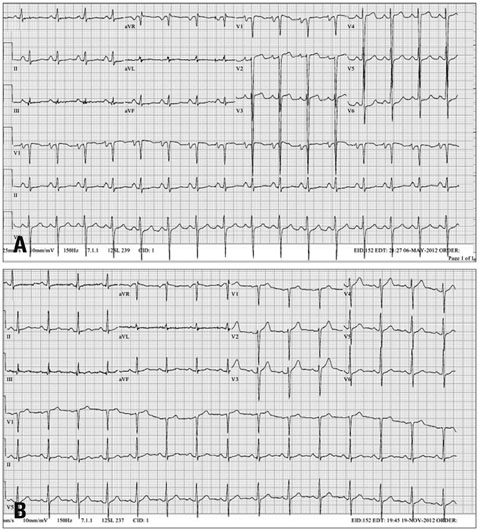
Fig. 2 Electrocardiogram findings. Electrocardiogram findings on admission (A) and at discharge (B).

Fig. 3 Chest X-ray and echocardiographic findings. Chest X-ray and echocardiographic findings before (A-D) and after treatment (E-H). Cardiomegaly and pulmonary infiltrates on chest X-ray, and left ventricular (LV) dysfunction on echocardiography were improved after 3 months of medical therapy. Asterisk (*) indicated LV thrombi.

Fig. 4 Magnetic resonance image findings of the heart. Magnetic resonance imaging of the heart reveals multiple high signal intensity in subepicardial and subendocardial area of left ventricular myocardium with multifocal delayed enhancement (arrowheads). Consolidative lesions with high signal intensity in right middle lobe were also noted (asterisk).
Cited by 1 articles
-
A pediatric case of eosinophilic granulomatosis with polyangiitis accompanied by heart failure mimicking an asthma attack
Min Jung Kim, Bo Ra Lee, Ji Soo Park, Yun Jung Choi, Mi Kyoung Song, Soyoung Lee, Dong In Suh
Allergy Asthma Respir Dis. 2019;7(4):212-217. doi: 10.4168/aard.2019.7.4.212.
Reference
-
1. Grau RG. Churg-Strauss syndrome: 2005-2008 update. Curr Rheumatol Rep. 2008; 10:453–458.2. Masi AT, Hunder GG, Lie JT, Michel BA, Bloch DA, Arend WP, Calabrese LH, Edworthy SM, Fauci AS, Leavitt RY, et al. The American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome (allergic granulomatosis and angiitis). Arthritis Rheum. 1990; 33:1094–1100.3. Solans R, Bosch JA, Pérez-Bocanegra C, Selva A, Huguet P, Alijotas J, Orriols R, Armadans L, Vilardell M. Churg-Strauss syndrome: outcome and long-term follow-up of 32 patients. Rheumatology (Oxford). 2001; 40:763–771.4. Aakerøy L, Amundsen BH, Skomsvoll JF, Haugen BO, Soma J. A 50-year-old man with eosinophilia and cardiomyopathy: need for endomyocardial biopsy. Eur J Echocardiogr. 2011; 12:257–259.5. Seo JS, Song JM, Kim DH, Kang DH, Song JK. A Case of Loeffler's Endocarditis Associated with Churg-Strauss Syndrome. J Cardiovasc Ultrasound. 2010; 18:21–24.6. Wolf J, Bergner R, Mutallib S, Buggle F, Grau AJ. Neurologic complications of Churg-Strauss syndrome--a prospective monocentric study. Eur J Neurol. 2010; 17:582–588.7. Abu-Shakra M, Smythe H, Lewtas J, Badley E, Weber D, Keystone E. Outcome of polyarteritis nodosa and Churg-Strauss syndrome. An analysis of twenty-five patients. Arthritis Rheum. 1994; 37:1798–1803.8. Finsterer J. Neurological manifestations of Churg-Strauss syndrome. Eur J Neurol. 2010; 17:524–525.9. Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S. Cardiac involvement in Churg-Strauss syndrome. Arthritis Rheum. 2010; 62:627–634.10. Szczeklik W, Miszalski-Jamka T, Mastalerz L, Sokolowska B, Dropinski J, Banys R, Hor KN, Mazur W, Musial J. Multimodality assessment of cardiac involvement in Churg-Strauss syndrome patients in clinical remission. Circ J. 2011; 75:649–655.11. Marmursztejn J, Vignaux O, Cohen P, Guilpain P, Pagnoux C, Gouya H, Mouthon L, Legmann P, Duboc D, Guillevin L. Impact of cardiac magnetic resonance imaging for assessment of Churg-Strauss syndrome: a cross-sectional study in 20 patients. Clin Exp Rheumatol. 2009; 27:1 Suppl 52. S70–S76.12. Mavrogeni S, Manoussakis MN, Karagiorga TC, Douskou M, Panagiotakos D, Bournia V, Cokkinos DV, Moutsopoulos HM. Detection of coronary artery lesions and myocardial necrosis by magnetic resonance in systemic necrotizing vasculitides. Arthritis Rheum. 2009; 61:1121–1129.13. Sliwa K, Damasceno A, Mayosi BM. Epidemiology and etiology of cardiomyopathy in Africa. Circulation. 2005; 112:3577–3583.14. Park JH, Kwon DH, Starling RC, Marwick TH. Role of imaging in the detection of reversible cardiomyopathy. J Cardiovasc Ultrasound. 2013; 21:45–55.15. Gharib MI, Burnett AK. Chemotherapy-induced cardiotoxicity: current practice and prospects of prophylaxis. Eur J Heart Fail. 2002; 4:235–242.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Churg-Strauss Syndrome with Endomyocardial Fibrosis
- A Case of Loeffler's Endocarditis Associated with Churg-Strauss Syndrome
- Cholecystectomy of a patient with Churg-Strauss syndrome: A case report
- A case of Churg-Strauss syndrome that underwent endoscopic sinus surgery under total intravenous anesthesia: A case report
- A Case of Churg-Strauss Syndrome Presenting Umbilicated Ulcerative Papules
