Two Cases of Optic Neuritis in Herpes Zoster Ophthalmicus
- Affiliations
-
- 1Department of Ophthalmology, Chonbuk National University, College of Medicine, Jeonju, Korea. ahnmin@chonbuk.ac.kr
- KMID: 2110888
- DOI: http://doi.org/10.3341/jkos.2008.49.6.1028
Abstract
-
PURPOSE: We report the treatment and prognosis of two patients who experienced pain in their face associated with skin lesions and acute decreased visual acuity and were diagnosed with optic neuritis caused by the herpes zoster virus.
CASE SUMMARY
Two patients were diagnosed with herpes zoster ophthalmicus after experiencing an acute decrease in visual acuity and were sent to our clinic for examination. On ophthalmic evaluation, the results were positive for relative afferent pupillary defect (RAPD) and showed abnormal VEP levels. On MRI T1, one case showed a high signal along the optic nerve sheath. Both patients with optic neuritis were treated with Acyclovir (Zovirax(R), GlaxoSmithKline, U.K.), which is an antiviral drug, at a dose of 10 mg/kg every 8 hours for 5 days, and a combination of prednisolone at a dose of 250 mg every 6 hours. After general therapy, they took Acyclovir (250 mg) orally 3 times daily for 14 days, with steroids (40 mg), and decreased the dosage after two weeks. We saw no improvement of visual acuity in either case, which still showed RAPD.
CONCLUSIONS
Optic neuritis secondary to herpes zoster ophthalmicus rarely occurs, but it is difficult to treat and has a poor prognosis. We should keep in mind that optic neuritis can occur in patients who were diagnosed with herpes zoster ophthalmicus.
Keyword
MeSH Terms
Figure
-
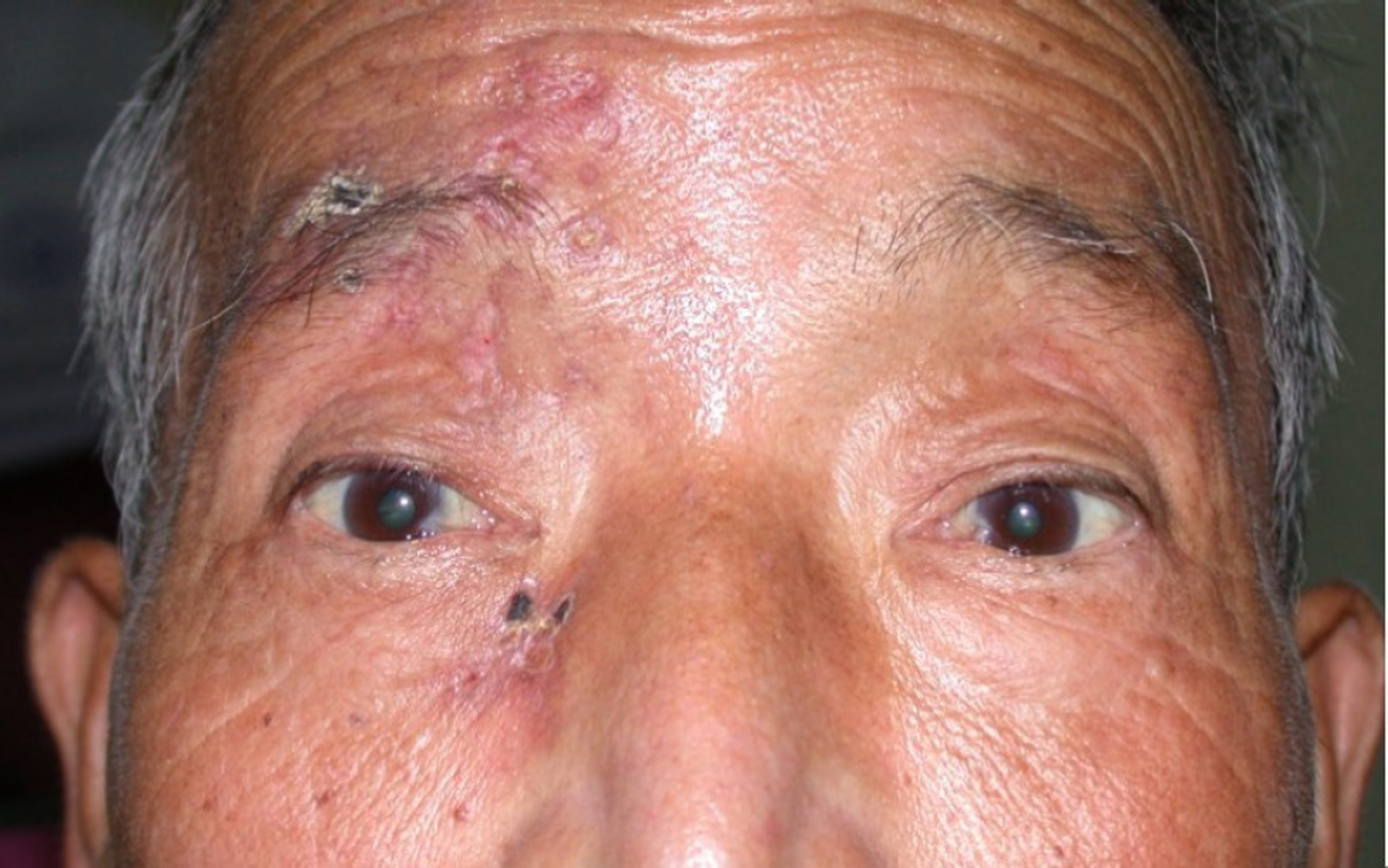
Figure 1. Skin eruptions corresponding to the dermatome of the left ophthalmic branch of the trigerminal nerve are seen.

Figure 2. VEP (visual evoked potential) study stimulating with LED-Goggle and recording from scalp showed absent evoked potential on the right side and acceptable valules on the left side.

Figure 3. Magnetic resonance imaging showed enlarged and well‐ enhanced right optic nerve sheath after contrast injection on T1 weighted sagittal image.

Figure 4. The blister formation and parasthesis on the right side of forehead was seen.
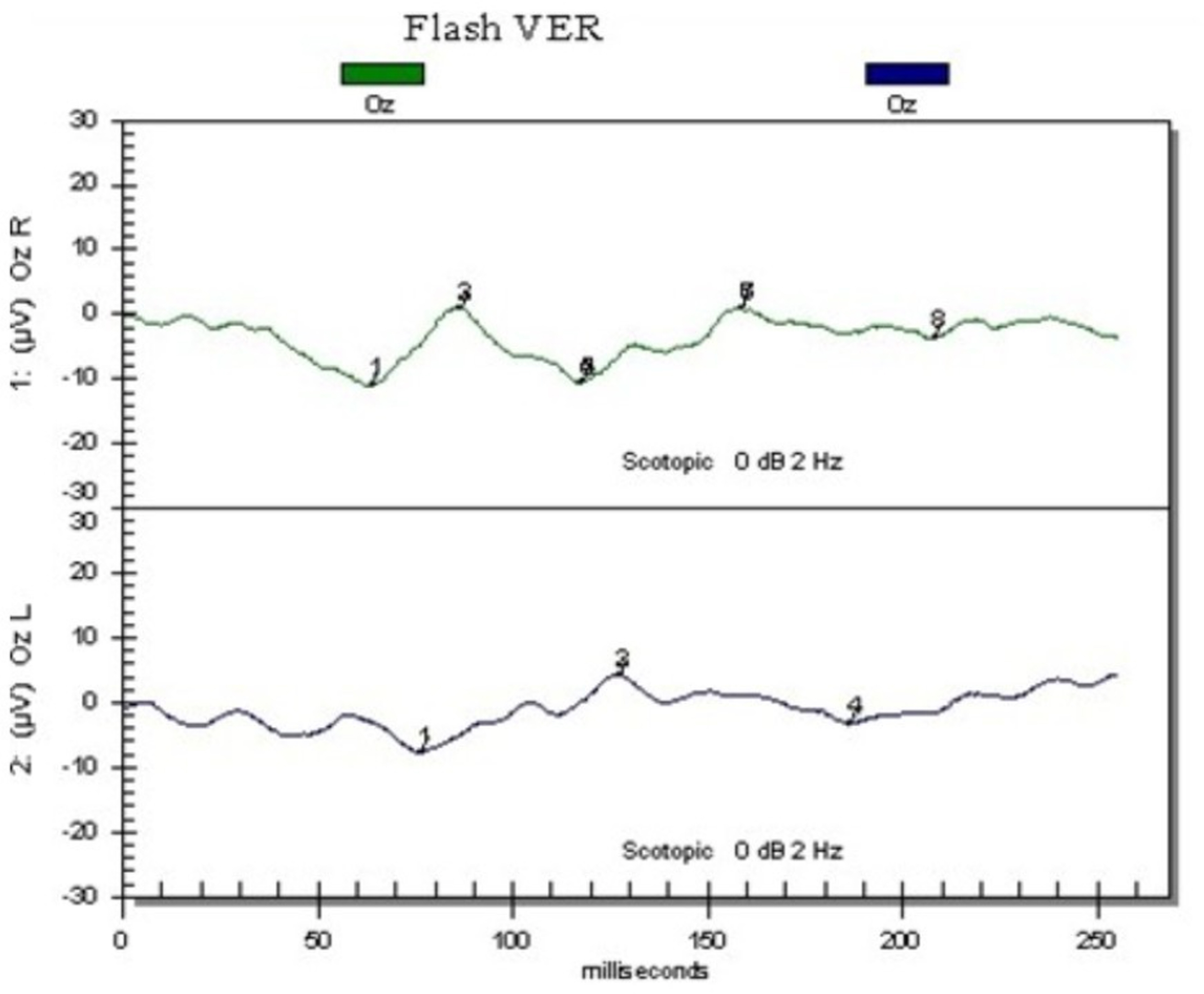
Figure 5. VEP (visual evoked potential) study. On the right side, the Latency of P2 was delayed and amplitude decreased. On the other side, the latency of P1, N1, P2 was delayed and amplitude decreased.
Cited by 5 articles
-
The Clinical Characteristics of Facial Herpes Zoster in Korean Patients
Hyun Joon Lee, So Young Kim, Moon Sun Jung
J Korean Ophthalmol Soc. 2010;51(1):8-13. doi: 10.3341/jkos.2010.51.1.8.Complicated Ophthalmopathy in Herpes Zoster Ophthalmicus Including Vitreous Opacity, Retinal Hemorrhage and Optic Neuropathy
Moses Kim, Mi Young Choi, Ju Byung Chae
J Korean Ophthalmol Soc. 2013;54(3):513-517. doi: 10.3341/jkos.2013.54.3.513.A Case of Multiple Complications in Herpes Zoster Ophthalmicus
Yeong Woo Son, Jin Hyun Kim, Seung Woo Lee
J Korean Ophthalmol Soc. 2015;56(5):789-793. doi: 10.3341/jkos.2015.56.5.789.Multiple Serous Chorioretinopathy after Facial Herpes Zoster
Sang Yoon Hyun, Dong Yoon Kim, Ju Byung Chae
J Korean Ophthalmol Soc. 2016;57(1):150-154. doi: 10.3341/jkos.2016.57.1.150.An Unusual Case of Orbital Inflammation Preceding Herpes Zoster Ophthalmicus
Ji Hyun Park, Ji Eun Lee
J Korean Ophthalmol Soc. 2017;58(9):1099-1105. doi: 10.3341/jkos.2017.58.9.1099.
Reference
-
References
1. Lee HR, Cho BC. A clinical study of herpes zoster ophthalmicus. J Korean Ophthalmol Soc. 1988; 29:387–91.2. Womack LW, Liesegang TJ. Complication of herpes zoster ophthalmicus. Arch Ophthalmol. 1983; 101:42–5.3. Duke-Elder, Stewart W.System of ophthalmology. Vol. 8. London: Medical Publisher and Booksiller;1965; 336–47.4. Cole EL, Meisler DM, Calabrese LH. . Herpes zoster ophthalmicus and acquired immune deficiency syndrome. Arch Ophthalmol. 1984; 102:1027–9.
Article5. Litoff D, Catalano RA. Herpes zoster optic neuritis in human immunedeficiency virus infection. Arch Ophthalmol. 1990; 108:782–3.6. Sandor EV, Millman A, Croxson TS, Mildvan D. Herpes zoster ophthalmicus in patients at risk for the acquired immune deficiency syndrome. Am J Ophthalmol. 1986; 101:153–5.7. Atmaca LS, Ozmert E. Optic neuropathy and central retinal artery occlusion in a patient with herpes zoster ophthalmicus. Ann Ophthalmol. 1992; 24:50–3.8. Borruat FX, Herbort CP. Herpes zoster ophthalmicus, anterior ischemic optic neuropathy and acyclovir. J Clin Neuro Ophthalmol. 1992; 12:37–40.9. Schmidt P. Herpes Zoster Ophthalmicus with retrobulbar neuritis. Acta Ophthalmol. 1983; 61:501–9.
Article10. Dhar MY, Goel JL, Sota LD. Optic neuroretinitis, a rare manifestation of herpes zoster ophthalmicus. J Commun Dis. 1997; 29:57–61.11. Kattah JC, Kennerdell JS. Orbital apex syndrome secondary to herpes zoster ophthalmicus. Am J Ophthalmol. 1978; 85:378–82.
Article12. Marsh RJ, Cooper M. Double‐ masked trial of topical acyclovir and steroids in the treatment of Herpes zoster ocular inflammation. Br J Ophthalmol. 1991; 75:542–6.13. Lexa FJ, Galetta SL, Yousem DM. . Herpes zoster Ophthalmicus with pseudotumor syndrome complicated by optic nerve infraction and cerebral granulomatous angiitis mr pathologic correlation. AJNR Am J Neuroradiol. 1993; 14:185–90.14. Winward KE, Hamed LM, Glaser JS. The spectrum of optic nerve disease in human immunodeficiency virus infection. Am J Ophthalmol. 1989; 107:373–80.
Article15. . . Complete ophthalmoplegia after ophthalmicus. J Neuroophthalmol. 1997; 17:262–5.16. Cobo LM, Foulk GN, Liesegang T. . Oral acyclovir in the therapy of acute herpes zoster ophthalmicus. Ophthalmology. 1985; 92:1547–83.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Herpes Zoster Ophthalmicus Complicated by Abducens Palsy
- A Case of Optic Neuritis Complicating Herpes Zoster Ophthalmicus in a Child
- Acute Vestibular Neuritis Associated with Herpes Zoster Ophthalmicus
- Complicated Ophthalmopathy in Herpes Zoster Ophthalmicus Including Vitreous Opacity, Retinal Hemorrhage and Optic Neuropathy
- Ophthalmoplegia in Herpes Zoster Ophthalmicus
