Status Epilepticus Caused by Small Amount Subacute to Chronic Subdural Hematoma: Case Report and Review of Literatures
- Affiliations
-
- 1Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. tdy815@hanmail.net
- KMID: 2106803
- DOI: http://doi.org/10.13004/jknts.2010.6.2.154
Abstract
- A 62-year-old man was admitted for focal seizure on the right perioral area and hand developed after minimal head trauma. Brain computed tomogram examination on admission showed small amount of chronic subdural hematoma on left fronto-parietal area. We planned conservative treatment with anticonvulsant, phenytoin. But, his seizure was sustained despite combination therapy of antiepileptic drugs including phenytoin and valproic acid, furthermore aggravated to complex partial seizure. Magnetic resonance image showed compression of motor cortex on the left hemisphere and electroencephalogram revealed seizure focus at the site of chronic subdural hematoma. He underwent craniotomy for hematoma evacuation, and operative field showed well demarcated margin between dark reddish hematoma and arachnoid membrane. However, his seizure was relapsed on 3rd postoperative day, and aggravated to "status epilepticus". The authors report this unusual case of status epilepticus from small amount of chronic subdural hematoma despite hematoma evacuation, and would like to emphasize early surgical intervention for the same cases.
MeSH Terms
Figure
-
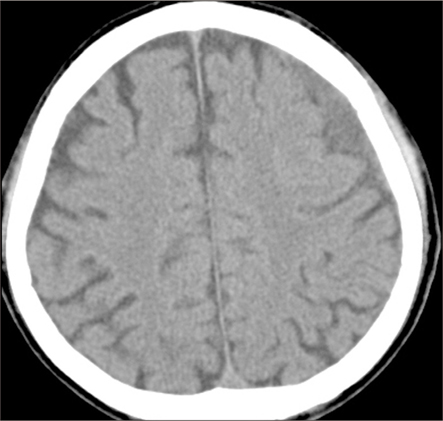
FIGURE 1 Admission head CT shows chronic subdural hematoma with slightly low density on the left fronto-parietal area. However, brain compression is not certain when compared with right side.
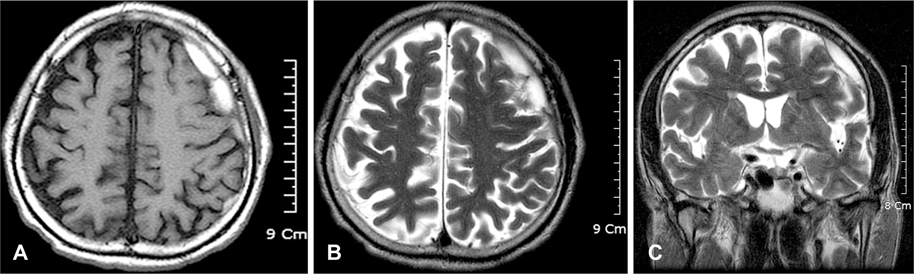
FIGURE 2 Preoperative brain magnetic resonance image (MRI) is checked up because of sustained seizure despite combination of anticonvulsant medications. Both T1-weighted image (A) and T2 weighted image (B) shows high signal intensity on the area prior to central sulcus with same nature like CT. However, coronal section (C) reveals more compressive lesion than admission CT scans. The degree of brain parenchymal compression may be underestimated at the CT.
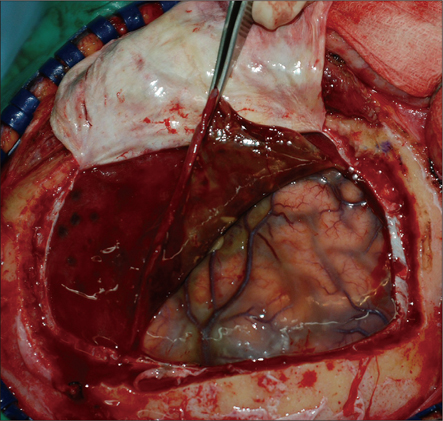
FIGURE 3 Intraoperative photograph. After dura is incised, dark reddish colored hematoma capsule is seen with well demarcated margin from arachnoid membrane and green tinged arachnoid membrane.
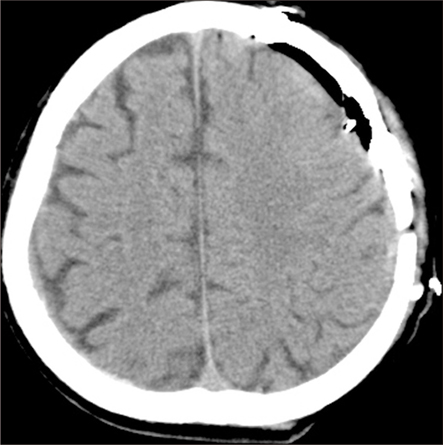
FIGURE 4 Immediate postoperative brain CT shows disappearance of hematoma, but slightly edematous change comparing with the right side.
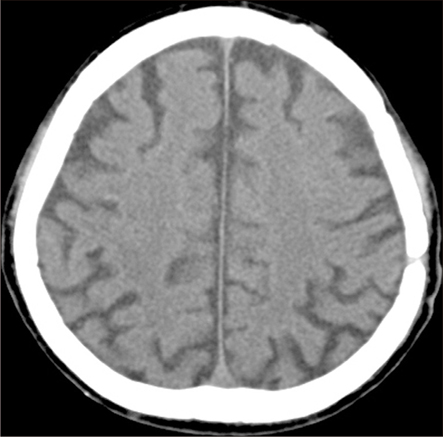
FIGURE 5 After three months, there is no structural abnormality on brain CT scan.
Reference
-
1. Brodersen P, Gjerris F. Regional cerebral flow in patients with chronic subdural hematomas. Acta Neurol Scand. 1975; 51:233–239.2. Cameron MM. Chronic subdural hematoma: a review of 114 cases. J Neurol Neurosurg Psychiatry. 1978; 41:834–839.3. Caveness WF. Epilepsy, a product of trauma in our time. Epilepsia. 1976; 17:207–215.
Article4. Chan AWK. Alcoholism and epilepsy. Epilepsia. 1985; 26:323–333.
Article5. Cole M, Spaz E. Seizures in chronic subdural hematoma. N Engl J Med. 1961; 265:628–631.
Article6. Drapkin AJ. Chronic subdural hematoma: pathophysiological basis for treatment. Br J Neurosurg. 1991; 5:467–473.
Article7. Hammond EJ, Ramsay RE, Villarral HJ, Wilder BJ. Effects of intracortical injection of blood and blood components on the electrocorticogram. Epilepsia. 1980; 21:3–14.
Article8. Jennett B. Early traumatic epilepsy. Incidence and significance after nonmissile injuries. Arch Neurol. 1974; 30:394–398.9. Chaves J, Sander JW. Seizure aggravation in idiopathic generalized epilepsies. Epilepsia. 2005; 46:Suppl 9. 133–139.
Article10. Kotwica Z, Brzeziński J. Chronic subdural haematoma treated by burr holes and closed system drainage: personal experience in 131 patients. Br J Neurosurg. 1991; 5:461–465.
Article11. Kotwica Z, Brzeziński J. [Early and late results of the surgical treatment of chronic subdural hematoma]. Neurol Neurochir Pol. 1987; 21:376–380.12. Kotwica Z, Brzeziński J. [Late results of surgical treatment of unilateral chronic subdural hematoma]. Pol Tyg Lek. 1988; 43:737–738.13. Ohno K, Suzuki R, Masaoka H, Matsushima Y, Inaba Y, Monma S. Role of traumatic subdural fluid collection in developing process of chronic subdural hematoma. Bull Tokyo Med Dent Univ. 1986; 33:99–106.14. Robinson RG. Chronic subdural hematoma: surgical management in 133 patients. J Neurosurg. 1984; 61:263–268.
Article15. Trojnar MK, Małek R, Chrościńska M, Nowak S, Błaszczyk B, Czuczwar SJ. Neuroprotective effects of antiepileptic drugs. Pol J Pharmacol. 2002; 54:557–566.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chronic Subdural Hematoma Superimposed on Posttraumatic Subdural Hygroma: A Report of Three Cases
- Probable Nonconvulsive Status Epilepticus after Drainage of a Chronic Subdural Hematoma in a Patient with Moyamoya Disease
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- Fatal Post-Operative Epilepticus after Burr-Hole Drainage for Chronic Subdural Hematoma
- Treatment of Chronic Subdural Hematoma with Arachnoid Cyst
