MR Imaging Features of Acute Enterovirus 71 Encephalitis in a Patient with Hand-Foot-Mouth Disease: A Case Report
- Affiliations
-
- 1Department of Radiology, Eulji University Hospital, Daejeon, Korea. midosyu@eulji.ac.kr
- KMID: 2097925
- DOI: http://doi.org/10.3348/jksr.2011.64.2.113
Abstract
- We report here on the MR findings of the first Korean case of hand-foot-mouth disease (HFMD) complicated by acute enterovirus 71 (EV 71) encephalitis in a 33-month old girl. Conventional MR images of the patient showed the increased signal intensity (SI) on a T2-weighted image (WI) at the posterior aspect of the medulla, the pontine tegmen, the bilateral dentate nuclei of the cerebellum and the midbrain. There was no evidence of abnormal SI or contrast enhancement at the same areas of the brain on the pre- and post-contrast T1-WI. The diffusion weighted images (DWI) also revealed the bilateral symmetrical strong high SI at the posterior aspect of the medulla and pontine tegmen and there was low SI at the same areas on the apparent diffusion coefficient (ADC) map. DWI in addition to the conventional MR imaging may be helpful for the early detection of acute EV 71 encephalitis in a patient with HFMD.
MeSH Terms
Figure
-
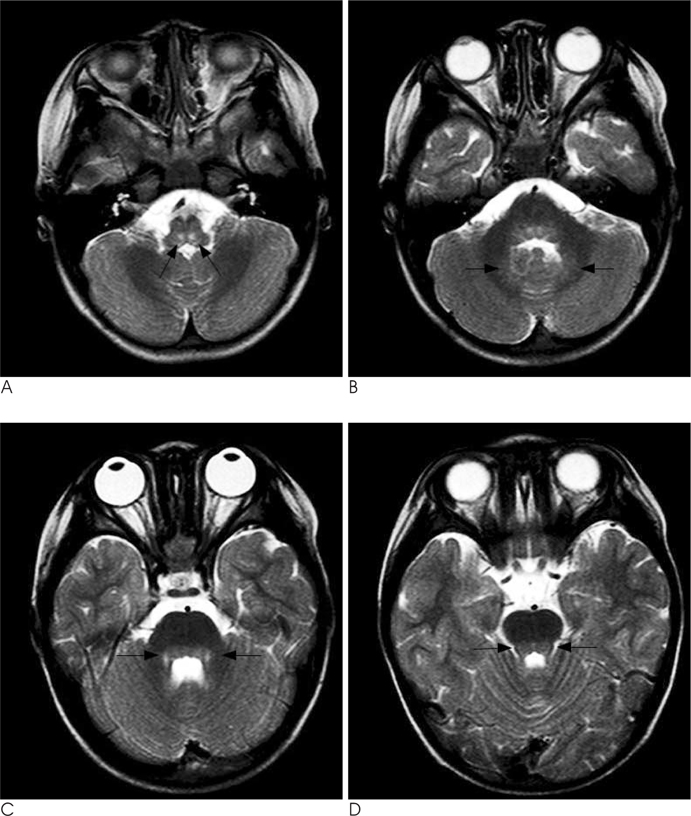
Fig. 1 A. The T2-weighted MR image reveals two symmetrical foci with focal high signal intensity (SI) at the posterior aspect of the medulla (arrows). B-D. The T2-weighted MR images of the brain stem level show bilateral multifocal foci with patchy increased SI (arrows) at the bilateral dentate nuclei of the cerebellum (B), the posterior aspect of the pons (C) and the midbrain (D).

Fig. 2 A. The T1-weighted MR image reveals no significant signal change at the posterior aspect of the medulla, and two symmetrical foci with focal high signal intensity (SI) (Fig. 1A) are seen on the T2-weightd image. B, C. The diffusion weighted image (DWI) (B) shows symmetrical strong high SI lesions at the posterior aspect of the medulla (arrows) with low SI on the ADC map (C) at the same areas (arrows). The DWI features reflect the reduced diffusivity and cytotoxic edema.
Reference
-
1. Kitamura A, Narisawa T, Hayashi A, Ashihara Y, Ishiko H, Minohara Y, et al. Serotype determination of enteroviruses that cause hand-foot-mouth disease: identification of enterovirus 71 and Coxsackievirus A16 from clinical specimens by using specific probe. Kansenshogaku Zasshi. 1997; 71:715–723.2. Wright PW, Strauss GH, Langford MP. Acute hemorrhagic conjunctivitis. Am Fam Physician. 1992; 45:173–178.3. Katiyar BC, Misra S, Singh RB, Singh AK, Gupta S, Gulati AK, et al. Adult polio-like syndrome following enterovirus 70 conjunctivitis (natural history of the disease). Acta Neurol Scand. 1983; 67:263–274.4. Yin-Murphy M, Baharuddin-Ishak , Phoon MC, Chow VT. A recent epidemic of Coxsackie virus type A24 acute haemorrhagic conjunctivitis in Singapore. Br J Ophthalmol. 1986; 70:869–873.5. Frieden IJ, Penneys NS. Viral infections. In : Schachner LA, Hansen RC, editors. Pediatric Dermatology. New York: Churchill Living Stone;1988. p. 1371–1413.6. Melnick JL. Enterovirus type 71 infections: a varied clinical pattern sometimes mimicking paralytic poliomyelitis. Rev Infect Dis. 1984; 6:Suppl 2. S387–S390.7. Nagy G, Takatsy S, Kukan E, Mihaly I, Domok I. Virological diagnosis of enterovirus type 71 infections: experiences gained during an epidemic of acute CNS diseases in Hungary in 1978. Arch Virol. 1982; 71:217–227.8. Shen WC, Chiu HH, Chow KC, Tsai CH. MR imaging findings of enteroviral encephalomyelitis: an outbreak in Taiwan. AJNR Am J Neuroradiol. 1999; 20:1889–1895.9. Sener RN. Herpes simplex encephalitis: diffusion MR imaging findings. Comput Med Imaging Graph. 2001; 25:391–397.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Enterovirus 71 Infection Presented with Acute Flaccid Paralysis
- Hand Foot Mouth Disease with Meningomyeloencephalitis Caused by Enterovirus 71
- A case of Enterovirus 71 Infection Presented with Acute Flaccid Paralysis in Jeju Island
- Enterovirus 71 Brainstem Encephalitis Presenting with Pulmonary Hemorrhage and Acute Heart Failure
- Hand, foot and mouth disease associated with the aseptic meningitis in Seoul, 1990
