Prevalence and Risk Factors for Erectile Dysfunction in Aging Men: Hallym Aging Study(HAS)
- Affiliations
-
- 1Department of Urology, Hallym University, Chunchon, Korea. sangklee@ hallym.ac.kr
- 2Institute for Aging Studies, School of Medicine, Hallym University, Chunchon, Korea.
- 3Department of Social Medicine, School of Medicine, Hallym University, Chunchon, Korea.
- KMID: 1990150
- DOI: http://doi.org/10.4111/kju.2007.48.12.1258
Abstract
-
PURPOSE: This study aims to estimate the prevalence of erectile dysfunction (ED) in a population-based sample of Korean men aged 45 or over, and to study its correlation with the socio-demographic, medical and lifestyle factors.
MATERIALS AND METHODS
385 men in Chunchon City were evaluated by clinical measures and questionnaires. All the participants were evaluated for erectile dysfunction. In conjunction with this evaluation, all the men were asked to complete the International Prostate Symptom Score(IPSS), and they underwent health examinations that included blood pressure, body mass index and waist-to-hip ratio, and the laboratory studies included the fasting blood glucose and total cholesterol levels. The subjects' medical history and health behaviors were investigated.
RESULTS
Out of the 385 men who visited our hospital, 285 completed the questionnaires. The prevalence of moderate or severe ED increased from 5.3% in men aged 45 to 54 years to 87.3% in men aged 75 or over. The standardized prevalence of ED was 41.5%. The IPSS were strongly correlated with ED(age adjusted partial R=??0.246, p<0.001). An increasing risk of ED was observed among those subjects with total cholesterol higher than 240mg/dl (adjusted odds ratio[aOR]=1.8), hypertension(aOR=2.2) and the ex-smokers(aOR=5.2). Education and family income were not correlated with ED(p>0.05).
CONCLUSIONS
The results of this community-based survey confirmed the strong correlation between advancing age and the prevalence of ED. Lower urinary tract symptoms are the major factors affecting erectile function. High blood pressure, high cholesterol levels and ex-smokers are significant risk factors for ED.
Keyword
MeSH Terms
Figure
-

Fig. 1. Prevalence of erectile dysfunction by age groups. The erectile dysfunction criteria were severe: International Index of Erectile Function-5 (IIEF-5) score≤10, moderate: 11-15, mild: 16-20 and normal: ≥21. The number in the box means the prevalence of erectile dysfunction, including severe, moderate and mild.
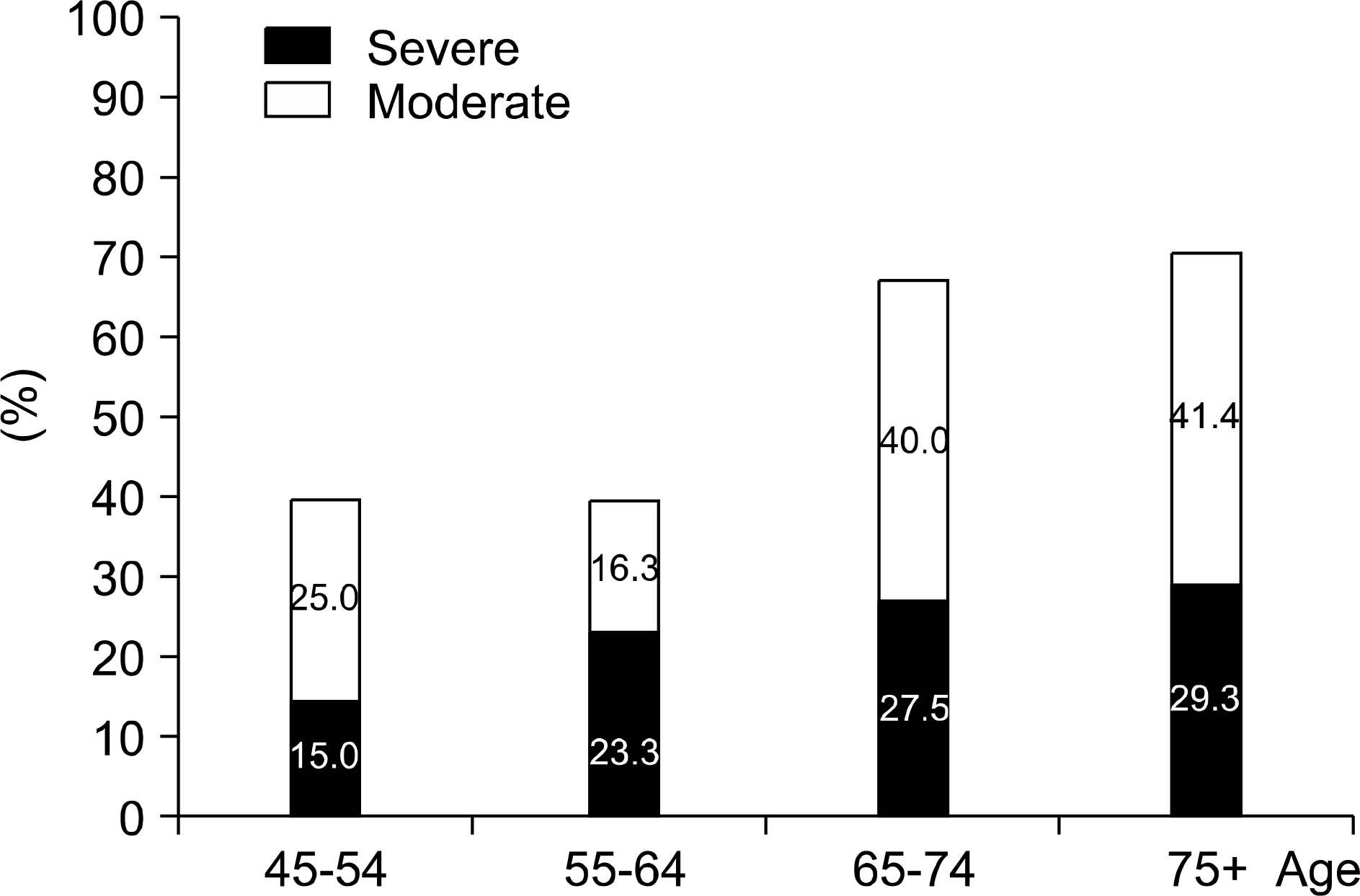
Fig. 2. Prevalence of low urinary tract symptom. The low urinary tract symptoms' criteria were severe: IPSS≥20 and moderate: 8-19, IPSS: International Prostate Symptom Score.

Fig. 3. International Index of Erectile Function-5 (IIEF-5) score and total cholesterol. Age adjusted partial Pearson's correlation coefficient: R= ?0.18 (p=0.044).
Cited by 1 articles
-
Comparison of pharmacokinetic characteristics of sildenafil citrate chewable tablets and film-coated tablets in healthy male subjects
Hyounggyoon Yoo, Sang Min Cho, Youn Woong Choi, Hye Jung Lee, Ji-Hye Kwon, Soo-Whan Kim, Jae Woo Kim, SeungHwan Lee, Jang-Hee Hong
Transl Clin Pharmacol. 2017;25(3):153-156. doi: 10.12793/tcp.2017.25.3.153.
Reference
-
1. Son H, Byun SS, Park E, Cho KS, Jo MK, Kim SW, et al. Prevalence of sexual dysfunction in men older than 40 living in Seoul: epidemiologic survey using questionnaire. Korean J Urol. 2002; 43:52–61.2. Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol. 1994; 151:54–61.
Article3. Bai Q, Xu QQ, Jiang H, Zhang WL, Wang XH, Zhu JC. Prevalence and risk factors of erectile dysfunction in three cities of China: a community-based study. Asian J Androl. 2004; 6:343–8.4. Roth A, Kalter-Leibovici O, Kerbis Y, Tenenbaum-Koren E, Chen J, Sobol T, et al. Prevalence and risk factors for erectile dysfunction in men with diabetes, hypertension, or both diseases: a community survey among 1,412 Israeli men. Clin Cardiol. 2003; 26:25–30.
Article5. Martin-Morales A, Sanchez-Cruz JJ, Saenz de Tejada I, Rodriguez-Vela L, Jimenez-Cruz JF, Burgos-Rodriguez R. Prevalence and independent risk factors erectile dysfunction in Spain: results of the epidemiologia de la disfunction erectile masculina study. J Urol. 2001; 166:569–74.6. Nehra A, Kulaksizoglu H. Global perspectives and contro-versies in the epidemiology of male erectile dysfunction. Curr Opin Urol. 2002; 12:493–6.
Article7. Blanker MH, Bosch JL, Groeneveld FP, Bohnen AM, Prins A, Thomas S, et al. Erectile and ejaculatory dysfunction in a community-based sample of men 50 to 78 years old: prevalence, concern, and relation to sexual activity. Urology. 2001; 57:763–8.
Article8. Vallancien G, Emberton M, Harving N, van Moorselaar RJ. Alf-One Study Group. Sexual dysfunction in 1,274 European men suffering from lower urinary tract symptoms. J Urol. 2003; 169:2257–61.
Article9. Braun MH, Sommer F, Haupt G, Mathers MJ, Reifenrath B, Engelmann UH. Lower urinary tract symptoms and erectile dysfunction: co-morbidity or typical ‘Aging Male' symptoms? Results of the ‘Cologne Male Survey'. Eur Urol. 2003; 44:588–94.
Article10. Kim SC. Hyperlipidemia and erectile dysfunction. Asian J Androl. 2000; 2:161–6.11. Lyngdorf P, Hemmingsen L. Epidemiology of erectile dysfunction and its risk factors: a practice-based study in Denmark. Int J Impot Res. 2004; 16:105–11.
Article12. Billups KL. Erectile dysfunction as an early sign of cardio-vascular disease. Int J Impot Res. 2005; 17(Suppl 1):S19–24.
Article13. Jeremy JY, Angelini GD, Khan M, Mikhailidis DP, Morgan RJ, Thompson CS, et al. Platelets, oxidant stress and erectile dysfunction: an hypothesis. Cardiovasc Res. 2000; 46:50–4.
Article14. Oh JY, Hong YS, Sung YA, Barrett-Connor E. Prevalence and factor analysis of metabolic syndrome in an urban Korean population. Diabetes Care. 2004; 27:2027–32.
Article15. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM. Development and evaluation of an bridged, 5-item version of the International Index of Erectile Dysfunction (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999; 11:319–26.16. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. the JNC 7 report. JAMA. 2003; 289:2560–72.
Article17. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2004; 27(Suppl 1):S5–10.18. Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults. Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adults treatment Panel III). JAMA. 2001; 285:2486–97.19. Khan MA, Thompson CS, Dashwood MR, Mumtaz FH, Morgan RJ, Mikhailidis DP. Endothelin-1 and nitric oxide in the pathogenesis of urinary tract disorders secondary to bladder outlet obstruction. Curr Vasc Pharmacol. 2003; 1:27–31.
Article20. Fung MM, Bettencourt R, Barrett-Connor E. Heart disease risk factors predict erectile dysfunction 25 years later. J Am Coll Cardiol. 2004; 43:1405–11.
Article21. Kupelian V, Shabsigh R, Araujo AB, O'Donnell AB, McKinlay JB. Erectile dysfunction as a predictor of the metabolic syndrome in aging men: results from the Massachusetts Male Aging Study. J Urol. 2006; 176:222–6.
Article22. McVary KT, Carrier S, Wessells H. Subcommittee on Smoking and Erectile Dysfunction, Socioeconomic Committee, Sexual Medicine Society of North America. Smoking and erectile dysfunction: evidence based analysis. J Urol. 2001; 166:1624–32.
Article23. Mirone V, Imbimbo C, Bortolotti A, Di Cintio E, Colli E, Landoni M, et al. Cigarette smoking as risk factor for erectile dysfunction: results from an Italian epidemiological study. Eur Urol. 2002; 41:294–7.
Article24. Austoni E, Mirone V, Parazzini F, Fasolo CB, Turchi P, Pescatori ES, et al. Smoking as a risk factor for erectile dysfunction: data from the Andrology Prevention Weeks 2001-2002 a study of the Italian Society of Andrology (s.l.a.). Eur Urol. 2005; 48:810–7.25. Shabsigh R, Fishman IJ, Schum C, Dunn JK. Cigarette smoking and other vascular risk factors in vasculogenic impotence. Urology. 1991; 38:227–31.26. Rosen MP, Greenfield AJ, Walker TG, Grant P, Dubrow J, Bettmann MA, et al. Cigarette smoking: an independent risk factor for atherosclerosis in the hypogastric-cavernous arterial bed of men with arteriogenic impotence. J Urol. 1991; 145:759–63.
Article27. Akkus E, Kadioglu A, Esen A, Doran S, Ergen A, Anafarta K, et al. Prevalence and correlates of erectile dysfunction in Turkey: a population-based study. Eur Urol. 2002; 41:298–304.
Article28. Lemere F, Smith JW. Alcohol-induced sexual impotence. Am J Psychiatry. 1973; 130:212–3.
Article29. Derby CA, Mohr BA, Goldstein I, Feldman HA, Johannes CB, McKinlay JB. Modifiable risk factors and erectile dysfunction: Can life style changes modify risk? Urology. 2000; 56:302–6.30. Esposito K, Giuqliano F, Di Palo C, Giuqliano G, Marfella R, D'Andrea F, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004; 291:2978–84.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prevalence and Risk Factors of Erectile Dysfunction in Diabetic Men by Self-Reported Questionnaires
- Association between Lower Urinary Tract Symptoms and Erectile Dysfunction in Aging Men: Hallym Aging Study
- Association between Erectile Dysfunction and Metabolic Syndrome in Aging Men: Hallym Aging Study
- Diagnosis and treatment of sexual dysfunction in elderly men
- Are Vascular Aging and Atherosclerosis Synonymous?
