Cyst Ablation Using a Mixture of N-Butyl Cyanoacrylate and Iodized Oil in Patients with Autosomal Dominant Polycystic Kidney Disease: the Long-Term Results
- Affiliations
-
- 1Department of Radiology, Seoul National University College of Medicine, Seoul 110-744, Korea. radjycho@radiol.snu.ac.kr
- 2Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul 110-744, Korea.
- 3Kidney Research Institute, Seoul National University Medical Research Center, Seoul 110-744, Korea.
- 4Department of Radiology, Keimyung University College of Medicine, Dongsan Medical Center, Daegu 700-712, Korea.
- KMID: 1777266
- DOI: http://doi.org/10.3348/kjr.2009.10.4.377
Abstract
OBJECTIVE
We wanted to assess the long-term results of cyst ablation with using N-butyl cyanoacrylate (NBCA) and iodized oil in patients with autosomal dominant polycystic kidney disease (ADPKD) and symptomatic cysts.
MATERIALS AND METHODS
Cyst ablation using a mixture of NBCA and iodized oil was performed in 99 cysts from 21 patients who had such symptoms as abdominal distension and pain. The collapse or reaccumulation of the ablated cysts after the procedure was assessed during the follow-up period of 36 to 90 months. The treatment effects, including symptom relief, and the clinical data such as the blood pressure and serum creatinine levels were also assessed, together with the complications.
RESULTS
The procedure was technically successful in all 99 cysts from the 21 patients. Any procedure-related significant complications were not detected. Seventy-seven of 99 cysts (78%) were successfully collapsed on the follow-up CT. Twenty-two cysts showed reaccumulation during long-term follow-up period. The clinical symptoms were relieved in 17 of the 21 patients (76%). Four of 12 patients (33%) with hypertension and two of six patients (33%) with azotemia were improved. End stage renal disease (ESRD) occurred in six of the 21 patients (28%) during the follow-up period. The mean age of ESRD in our patients was 57 years. The mean time interval for the development of ESRD was 19 months.
CONCLUSION
Ablation using a mixture of NBCA and iodized oil may be an effective, safe method for obtaining symptom relief in patients with ADPKD.
MeSH Terms
Figure
-
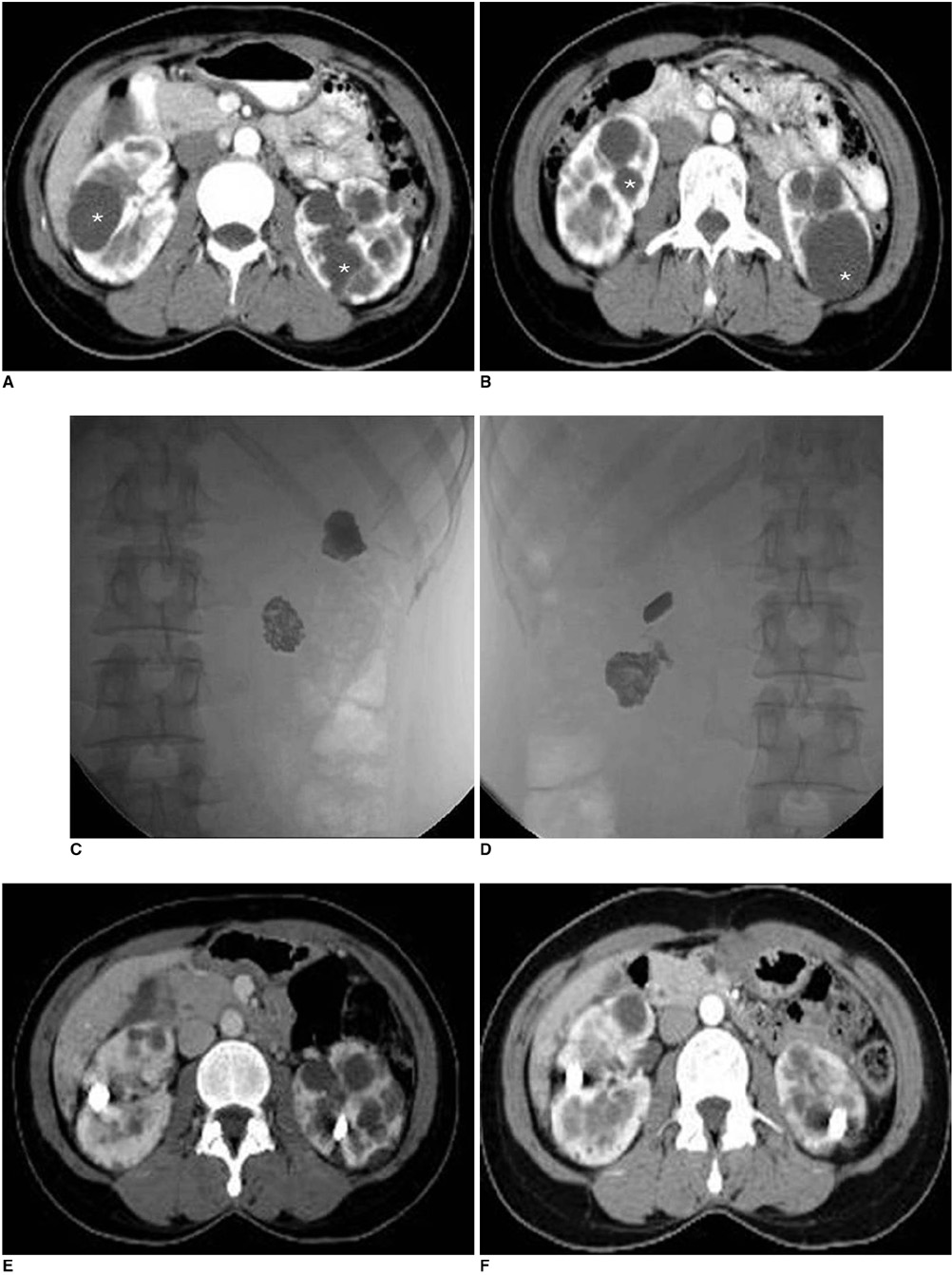
Fig. 1 36-year-old woman with autosomal dominant polycystic kidney disease. A, B. Axial contrast enhanced CT scans show multiple cysts in both kidneys. Cyst ablation was performed for two cysts in right kidney and for two cysts in left kidney (asterisk). C, D. Antero-posterior radiographies after procedure show lobulated radiopacities that represent mixture of N-butyl cyanoacrylate and iodized oil in right (C) and left (D) kidneys. E. Follow-up CT scans 36 months after procedure show collapsed cysts with mixture of N-butyl cyanoacrylate and iodized oil. F. Follow-up CT scans at 60 months show no evidence of reaccumulation in ablated cysts.
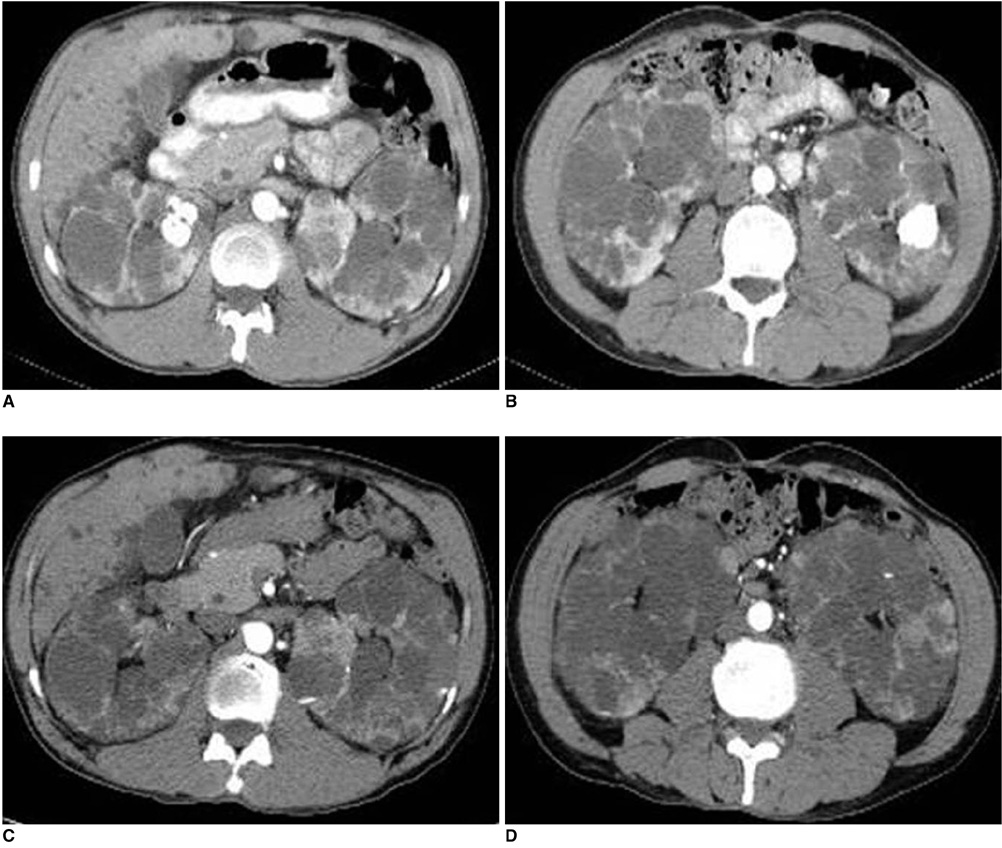
Fig. 2 52-year-old man with autosomal dominant polycystic kidney disease and who underwent cyst ablation. A, B. Follow-up CT scans 24 month later show radiopacities within ablated cysts. C, D. Follow-up CT scans at 50 month show reaccumulation of cystic fluid.
Cited by 1 articles
-
Predictors of the Frequency of Ethanol Injections for Renal Cyst Ablation: A Preliminary Study
Yong Hun Kim, Bum Sang Cho
J Korean Soc Radiol. 2018;78(3):193-199. doi: 10.3348/jksr.2018.78.3.193.
Reference
-
1. Schwenger V, Zeier M. Autosomal dominant polycystic kidney disease. Saudi J Kidney Dis Transpl. 1999. 10:7–20.2. Gabow PA. Autosomal dominant polycystic kidney disease. N Engl J Med. 1993. 329:3323–3342.3. Torres VE, Harris PC, Pirson Y. Autosomal dominant polycystic disease. Lancet. 2007. 369:1287–1301.4. Segal AJ, Spataro RF. Computed tomography of adult polycystic disease. J Comput Assist Tomogr. 1982. 6:777–780.5. Choyke PL. Inherited cyst disease of the kidney. Radiol Clin North Am. 1996. 34:925–946.6. Terada N, Ichioka K, Matsuta Y, Okubo K, Yoshimura K, Arai Y. The natural history of simple renal cysts. J Urol. 2002. 167:21–23.7. Hayden CK Jr, Swischuk LE. Renal cystic disease. Semin Ultrasound CT MR. 1991. 12:361–373.8. Hartman DS. Renal cystic disease in multisystem conditions. Urol Radiol. 1992. 14:13–17.9. Romao EA, Moyses Neto M, Teixeira SR, Muglia VF, Vieira-Neto OM, Dantas M. Renal and extrarenal manifestations of autosomal dominant polycystic kidney disease. Braz J Med Biol Res. 2006. 39:533–538.10. Bennett WM, Elzinga L, Golper TA, Barry JM. Reduction of cyst volume for symptomatic management of autosomal dominant polycystic kidney disease. J Urol. 1987. 137:620–622.11. Elzinga LW, Barry JM, Torres VE, Zincke H, Wahner HW, Swan S, et al. Cyst decompression surgery for autosomal dominant polycystic kidney disease. J Am Soc Nephrol. 1992. 2:1219–1226.12. Pirson Y. Recent advances in the clinical management of autosomal-dominant polycystic kidney disease. QJM. 1996. 89:803–806.13. Bajwa ZH, Gupta S, Warfield CA, Steinman TI. Pain management in polycystic kidney disease. Kidney Int. 2001. 60:1631–1644.14. Wilson PD, Guay-Woodford L. Pathophysiology and clinical management of polycystic kidney disease in woman. Semin Nephrol. 1999. 19:123–132.15. Gibson P, Watson ML. Cyst infection in polycystic kidney disease: a clinical challenge. Nephrol Dial Transplant. 1998. 13:2455–2457.16. Chapman AB, Thickman D, Gabow PA. Percutaneous cyst puncture in the treatment of cyst infection in autosomal dominant polycystic kidney disease. Am J Kidney Dis. 1990. 16:252–255.17. Hanna RM, Dahniya MH. Aspiration and sclerotherapy of symptomatic simple renal cysts: value of two injections of sclerosing agents. AJR Am J Roentgenol. 1996. 167:781–783.18. Fontana D, Porpiglia F, Morra I, Destefanis P. Treatment of simple renal cysts by percutaneous drainage with three repeated injection. Urology. 1999. 53:904–907.19. Chung BH, Kim JH, Hong CH, Yang SC, Lee MS. Comparison of single and multiple session of percutaneous sclerotherapy for renal cyst. BJU Int. 2000. 85:626–627.20. Seo TS, Oh JH, Yoon Y, Lim JW, Park SJ, Chang SG, et al. Acetic acid as a sclerosing agent for renal cysts: comparison with ethanol in follow-up results. Cardiovasc Intervent Radiol. 2000. 23:177–181.21. Uemasu J, Fugihara M, Munemura C, Nakamura E, Kawasaki H. Cyst sclerotherapy with minocycline hydrochrolide in patients with autosomal dominant polycystic kidney disease. Nephrol Dial Transplant. 1996. 11:843–846.22. Peyromaure M, Debre B, Flam TA. Sclerotherapy of a giant renal cyst with povidone-iodine. J Urol. 2002. 168:2525.23. Kim JH, Lee JT, Kim EK, Won JY, Kim MJ, Lee JD, et al. Percutaneous sclerotherapy of renal cysts with a beta-emitting radionuclide, holmium-166-chitosan complex. Korean J Radiol. 2004. 5:128–133.24. Bean WJ. Renal cysts: treatment with alcohol. Radiology. 1981. 138:329–331.25. el-Diasty TA, Shokeir AA, Tawfeek HA, Mahmoud NA, Nabeeh A, Ghoneim MA. Ethanol sclerotherapy for symptomatic simple renal cysts. J Endourol. 1995. 9:273–276.26. Bozkurt FB, Boyvat F, Tekin I, Aytekin C, Coskun M, Ozkardes H. Percutaneous sclerotherapy of a giant benign renal cyst with alcohol. Eur J Radiol. 2001. 40:64–67.27. Lee YR, Lee KB. Ablation of symptomatic cysts using absolute ethanol in 11 patients with autosomal-dominant polycystic kidney disease. Korean J Radiol. 2003. 4:239–242.28. Suh DC, Shi HB, Park SS, Lee MS, Choi HY. Change of spontaneous reaction of glue and lipiodol mixture during embolization after the addition of tungsten powder: in vitro study. AJNR Am J Neuroradiol. 2000. 21:1277–1279.29. Kim SH, Moon MW, Lee HJ, Sim JS, Kim SH, Ahn C. Renal cyst ablation with n-butyl cyanolate and iodized oil in symptomatic patients with autosomal dominant polycystic kidney disease: preliminary report. Radiology. 2003. 226:573–576.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of renal arterial embolization using 99% ethanol and lipiodol mixture for autosomal dominant polycystic kidney disease in a hemodialysis patient
- Sclerotherapy of Renal Cysts in Korean ADPKD Patients
- A Case of Renal Cell Carcinoma in Autosomal Dominant Polycystic Kidney Disease Hemodialyzed
- Ablation of Symptomatic Cysts Using Absolute Ethanol in 11 Patients with Autosomal-Dominant Polycystic Kidney Disease
- A Case Report: Prenatal Ultrasonographic Diagnosis of Autosomal Dominant Polycystic Kidney Disease
