Cancer Res Treat.
2007 Sep;39(3):104-108.
Bone Metastasis from Primary Hepatocellular Carcinoma: Characteristics of Soft Tissue Formation
- Affiliations
-
- 1Department of Radiation Oncology, Ajou University School of Medicine, Suwon, Korea. chunm@ajou.ac.kr
- 2Department of Surgery, Ajou University School of Medicine, Suwon, Korea.
- 3Department of Internal Medicine, Ajou University School of Medicine, Suwon, Korea.
Abstract
-
PURPOSE: To assess the characteristics of bone metastasis from hepatocellular carcinoma and the radiation field arrangement based on imaging studies.
MATERIALS AND METHODS
Fifty-three patients (84 lesions) with bone metastasis from a primary hepatocellular carcinoma completed palliative radiation therapy. All patients underwent one of following imaging studies prior to the initiation of radiation therapy: a bone scan, computed tomography or magnetic resonance imaging. The median radiation dose was 30 Gy (7~40 Gy). We evaluated retrospectively the presence of soft tissue formation and the adjustment of the radiation field based on the imaging studies.
RESULTS
Soft tissue formation at the site of bony disease was identified from either a CT/MRI scan (41 lesions) or from a symptomatic palpable mass (5 lesions). The adjustment of the radiation field size based on a bone scan was necessary for 31 of 41 soft tissue forming lesions (75.6%), after a review of the CT/MRI scan. The median survival from the initial indication of a hepatoma diagnosis was 8 months (2 to 71 months), with a 2-year survival rate of 38.6%. The median survival from the detection of a bone metastasis was 5 months (1 to 38 months) and the 1-year overall survival rate was 8.7%.
CONCLUSION
It was again identified that bone metastasis from a primary hepatocellular carcinoma is accompanied by soft tissue formation. From this finding, an adjustment of the radiation field size based on imaging studies is required. It is advisable to obtain a CT or MRI scan of suspected bone metastasis for better tumor volume coverage prior to the initiation of radiation therapy.
MeSH Terms
Figure
-
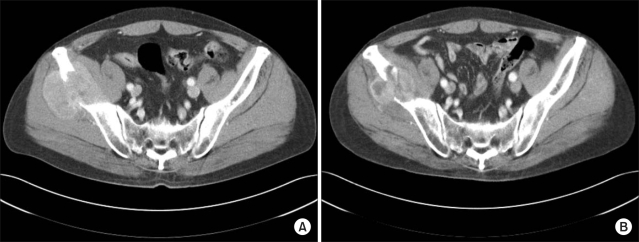
Fig. 1 (A) The pre-treatment CT scan shows osteolysis of the right iliac wing by soft tissue formation. (B) The mass size decreases 2 months after completion of radiation therapy with persistent bony destruction.
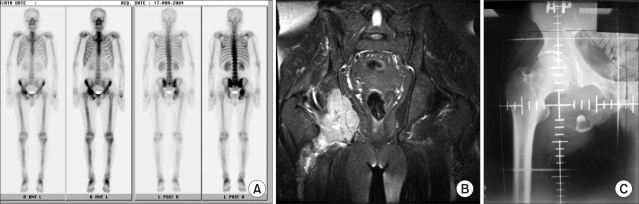
Fig. 2 A bone scan (A) and pelvic MRI (B) of a 46-year-old male patient. Note the osteolytic lesion with expansile soft tissue formation on the right iliac bone. (C) The difference of radiation field based on the bone scan and MRI of the pelvis.
Reference
-
1. Park JW, Kim CM. Epidemiology of hepatocellular carcinoma in Korea. Korean J Hepatol. 2004; 11:303–310. PMID: 16380659.2. Llovet JM, Real MI, Montana X, Planas R, Coll S, Aponte J, et al. Arterial embolisation or chemoembolisation, versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: a randomized trial. Lancet. 2002; 359:1734–1739. PMID: 12049862.3. Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasegawa H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment: study of 850 patients. Cancer. 1985; 56:918–928. PMID: 2990661.
Article4. The Liver Cancer Study Group of Japan. Primary liver cancer in Japan: Sixth report. Cancer. 1987; 60:1400–1411. PMID: 3040216.5. Okazaki N, Yoshino M, Yoshida T, Hirohashi S, Kishi K, Shimosato Y. Bone metastasis in hepatocellular carcinoma. Cancer. 1985; 55:1991–1994. PMID: 2983871.
Article6. Lee YT, Geer DA. Primary liver cancer: pattern of metastasis. J Surg Oncol. 1987; 36:26–31. PMID: 3041113.
Article7. Fukutomi M, Yokota M, Chuman H, Harada H, Zaitsu Y, Funakoshi A, et al. Increased incidence of bone metastasis in hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2001; 13:1083–1088. PMID: 11564960.8. Johnson PJ. Is there a role for systemic therapy in hepatocellular carcinoma, and if so, can we assess response? 2002. 38:Am Soc Clin Oncol;p. 310–315. Ed Book.9. Seong J, Koom WS, Park HC. Radiotherapy for painful bone metastasis from hepatocellular carcinoma. Liver Int. 2005; 25:261–265. PMID: 15780048.10. Kaizu YT, Karasawa K, Tanaka Y, Matuda T, Kurosaki H, Tanaka S, et al. Radiotherapy for osseous metastasis from hepatocellular carcinoma: a retrospective study of 57 patients. Am J Gastroenterol. 1998; 93:2167–2171. PMID: 9820391.11. Sato M, Ishida H, Konno K, Hamashima Y, Naganuma H, Komatsuda T, et al. Peripheral bone metastasis from hepatocellular carcinoma: sonographic findings. Abdom Imaging. 2001; 26:524–528. PMID: 11503093.
Article12. Goilimbu C, Firooznia H, Rafii M. Hepatocellular carcinoma with skeletal metastasis. Radiology. 1985; 154:617–618. PMID: 2982174.
Article13. Kuhlman JE, Fishman EK, Leichner PK, Magid D, Order SE, Siegelman SS. Skeletal metastasis from hepatoma: frequency, distribution and radiographic features. Radiology. 1986; 160:175–178. PMID: 3012630.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Bone Metastasis from Hepatocellular Carcinoma Using 18F-FDG PET/CTand 99mTc-HDP Bone Scintigraphy: Characteristics of Soft Tissue Formation
- Metastatic hepatocellular carcinoma in the maxilla and temporal bone: a rare case report
- Unusual Semimembranosus Muscle Metastasis from Hepatocellular Carcinoma
- Two Cases of Cutaneous Metastasis Originating from Hepatocellular Carcinoma
- Pulmonary metastasis of primary hepatocellular carcinoma
