Clinical Features of Idiopathic Juxtafoveal Telangiectasis in Koreans
- Affiliations
-
- 1Department of Ophthalmology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. swkang@skku.edu
- 2Department of Ophthalmology, Dongguk University College of Medicine, Gyeongju, Korea.
- KMID: 1018408
- DOI: http://doi.org/10.3341/kjo.2011.25.4.225
Abstract
- PURPOSE
To describe the clinical characteristics of idiopathic juxtafoveal telangiectasis (IJT) in Koreans.
METHODS
Medical records of 16 patients with IJT were analyzed during the period from 1997 to 2009. Diagnosis was based on biomicrosopic and fluorescein angiographic findings and the group was determined according to the Gass and Blodi classification.
RESULTS
We analyzed eight patients in group 1A (50%), two in group 1B (12.5%), and six in group 2A (37.5%). Diverse treatment modalities, such as macular laser photocoagulation, photodynamic therapy, intravitreal antiangiogenic agent, and steroid injection, were applied for macular edema in nine eyes; however, only two eyes showed visual improvement.
CONCLUSIONS
In this case series, group 1A was the most common. For macular edema related to IJT, current treatment strategies had no consistent effect.
Keyword
MeSH Terms
-
Adolescent
Adult
Aged
Angiogenesis Inhibitors/administration & dosage
Child
Female
Fluorescein Angiography
Follow-Up Studies
Fovea Centralis/*blood supply
Fundus Oculi
Glucocorticoids/administration & dosage
Humans
Incidence
Intravitreal Injections
Male
Microscopy, Acoustic
Middle Aged
Photochemotherapy/methods
Prognosis
Republic of Korea/epidemiology
Retinal Diseases/*diagnosis/drug therapy/epidemiology
Retinal Vessels/*pathology/ultrasonography
Retrospective Studies
Risk Factors
Telangiectasis/*diagnosis/drug therapy/epidemiology
Visual Acuity
Young Adult
Figure
-

Fig. 1 Group 1A idiopathic juxtafoveal retinal telangiectasis (case 12). (A) Color fundus photography of the left eye on presentation showed a lipid exudate with aneurysm-like capillaries in its center. (B) Fluorescein angiography of the left eye on presentation showed telangiectasis and microaneurysm. (C) Optical coherence tomography of the left eye on presentation indicates macular edema with foveolar detachment. (D) Macular edema showed no improvement 3 months after a repeat intravitreal bevacizumab treatment and focal laser photocoagulation.

Fig. 2 Group 1B idiopathic juxtafoveal retinal telangiectasis (case 6). (A) Color fundus photography of the right eye on presentation. (B) Fluorescein angiography of the right eye on presentation showed focal juxtafoveal telangiectasis. (C) Optical coherence tomography of the right eye on presentation. Images demonstrated a foveal cystoid and intraretinal edema. (D) The macular edema resolved after photodynamic treatment.
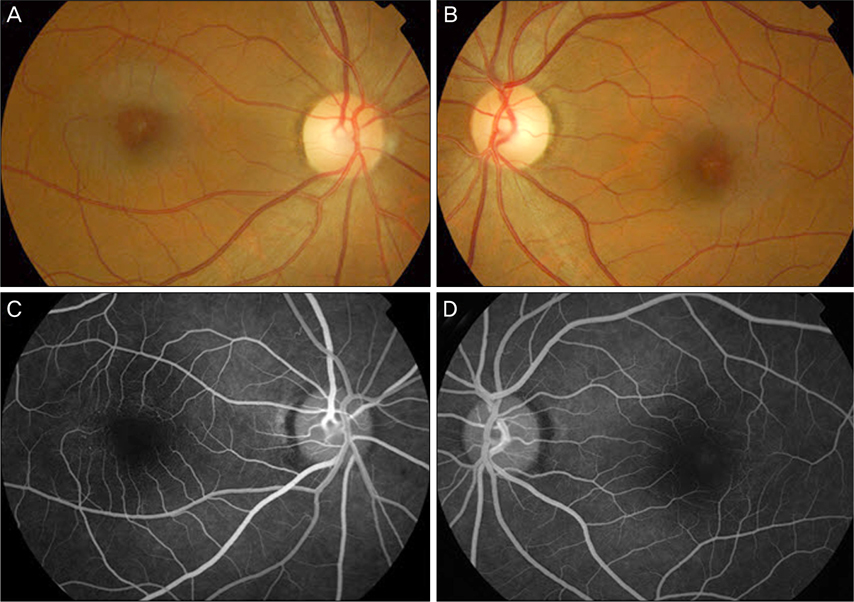
Fig. 3 Group 2A idiopathic juxtafoveal retinal telangiectasis (case 10) (A,B) Color fundus photography of both eyes on presentation showed slight graying of the perifoveal retina and lipid exudates in the right eye. (C,D) Fluorescein angiography of both eyes on presentation showed telangiectatic change in the temporal macular lesion.
Cited by 1 articles
-
A Case of Bilateral Macular Hole in a Patient with Bilateral Macular Telangiectasia
Suk Jin Kim, Ki Seok Kim
J Korean Ophthalmol Soc. 2013;54(9):1458-1462. doi: 10.3341/jkos.2013.54.9.1458.
Reference
-
1. Gass JD, Oyakawa RT. Idiopathic juxtafoveolar retinal telangiectasis. Arch Ophthalmol. 1982. 100:769–780.2. Gass JD, Blodi BA. Idiopathic juxtafoveolar retinal telangiectasis. Update of classification and follow-up study. Ophthalmology. 1993. 100:1536–1546.3. Chang YI, Lee JG, Kim TW, Lee EK. The Clinical manifestations and treatments of parafoveal telangiectasis. J Korean Ophthalmol Soc. 2004. 45:576–584.4. Park DW, Schatz H, McDonald HR, Johnson RN. Grid laser photocoagulation for macular edema in bilateral juxtafoveal telangiectasis. Ophthalmology. 1997. 104:1838–1846.5. Kotoula MG, Chatzoulis DZ, Karabatsas CH, et al. Resolution of macular edema in idiopathic juxtafoveal telangiectasis using PDT. Ophthalmic Surg Lasers Imaging. 2009. 40:65–67.6. Smithen LM, Spaide RF. Photodynamic therapy and intravitreal triamcinolone for a subretinal neovascularization in bilateral idiopathic juxtafoveal telangiectasis. Am J Ophthalmol. 2004. 138:884–885.7. Alldredge CD, Garretson BR. Intravitreal triamcinolone for the treatment of idiopathic juxtafoveal telangiectasis. Retina. 2003. 23:113–116.8. Wu L, Evans T, Arevalo JF, et al. Long-term effect of intravitreal triamcinolone in the nonproliferative stage of type II idiopathic parafoveal telangiectasia. Retina. 2008. 28:314–319.9. Charbel Issa P, Holz FG, Scholl HP. Findings in fluorescein angiography and optical coherence tomography after intravitreal bevacizumab in type 2 idiopathic macular telangiectasia. Ophthalmology. 2007. 114:1736–1742.10. Kovach JL, Rosenfeld PJ. Bevacizumab (avastin) therapy for idiopathic macular telangiectasia type II. Retina. 2009. 29:27–32.11. Maia OO Jr, Bonanomi MT, Takahashi WY, et al. Intravitreal bevacizumab for foveal detachment in idiopathic perifoveal telangiectasia. Am J Ophthalmol. 2007. 144:296–299.12. Moon SJ, Berger AS, Tolentino MJ, Misch DM. Intravitreal bevacizumab for macular edema from idiopathic juxtafoveal retinal telangiectasis. Ophthalmic Surg Lasers Imaging. 2007. 38:164–166.13. Gass JD. A fluorescein angiographic study of macular dysfunction secondary to retinal vascular disease. V. Retinal telangiectasis. Arch Ophthalmol. 1968. 80:592–605.14. Tripathi R, Ashton N. Electron microscopical study of Coat's disease. Br J Ophthalmol. 1971. 55:289–301.15. Abujamra S, Bonanomi MT, Cresta FB, et al. Idiopathic juxtafoveolar retinal telangiectasis: clinical pattern in 19 cases. Ophthalmologica. 2000. 214:406–411.16. Watzke RC, Klein ML, Folk JC, et al. Long-term juxtafoveal retinal telangiectasia. Retina. 2005. 25:727–735.17. Yannuzzi LA, Bardal AM, Freund KB, et al. Idiopathic macular telangiectasia. Arch Ophthalmol. 2006. 124:450–460.18. Aung KZ, Wickremasinghe SS, Makeyeva G, et al. The prevalence estimates of macular telangiectasia type 2: the Melbourne Collaborative Cohort Study. Retina. 2010. 30:473–478.19. Klein R, Blodi BA, Meuer SM, et al. The prevalence of macular telangiectasia type 2 in the Beaver Dam eye study. Am J Ophthalmol. 2010. 150:55–62.e2.20. Chew EY, Murphy RP, Newsome DA, Fine SL. Parafoveal telangiectasis and diabetic retinopathy. Arch Ophthalmol. 1986. 104:71–75.21. Millay RH, Klein ML, Handelman IL, Watzke RC. Abnormal glucose metabolism and parafoveal telangiectasia. Am J Ophthalmol. 1986. 102:363–370.22. Charbel Issa P, Finger RP, Holz FG, Scholl HP. Eighteen-month follow-up of intravitreal bevacizumab in type 2 idiopathic macular telangiectasia. Br J Ophthalmol. 2008. 92:941–945.23. Gamulescu MA, Walter A, Sachs H, Helbig H. Bevacizumab in the treatment of idiopathic macular telangiectasia. Graefes Arch Clin Exp Ophthalmol. 2008. 246:1189–1193.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Macular Hole in a Patient with Bilateral Macular Telangiectasia
- Demographic Features of Idiopathic Macular Telangiectasia in Korean Patients
- Long-term Natural Course of Idiopathic Choroidal Neovascularization
- ICGA Findings and Clinical Features of Idiopathic Choroidal Neovascularization
- Combination Therapy with Photodynamic Therapy and Intravitreal Bevacizumab in Idiopathic Macular Telangiectasia Type I
