Radiologic-Pathologic Correlation of Unusual Lingual Masses:Part I: Congenital Lesions
- Affiliations
-
- 1Seoul Natl Univ Hosp,Dept Diagnost Radiol Chongno Gu,28 Yongon Dong, Seoul 110744, South Korea.
- KMID: 754121
- DOI: http://doi.org/10.3348/kjr.2001.2.1.37
Abstract
- Because the tongue is superficially located and the intial manifestation of most diseases occurring there is mucosal change, lingual these lesions can be easily accessed and diagnosed without imaging analysis. Most congenital lesions of the tongue, however, can manifest as a submucosal bulge and be located in a deep portion of that organ such as its base; their true characteristics and extent may be recognized only on cross-sectional images such as those obtained by CT or MRI. In addition, because it is usually difficult to differentiate congenital lesions from other submucosal neoplasms on the basis of imaging findings alone, clinical history and physical examination should always be taken into consideration when interpretating CT and MR images of the tongue. Although the radiologic findings for congenital lesions are nonspecific, CT and MR imaging can play an important role in the diagnostic work-up of these unusual lesions. Delineation of the extent of the tumor, and recognition and understanding of the spectrum of imaging and the pathologic features of these lesions, often help narrow the differential diagnosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 Lingual thyroid in a 31-year-old man with mild dyspnea. A. Contrast-enhanced axial CT scan shows a well-marginated, homogeneously enhancing mass without evidence of cystic change or calcification at the dorsal aspect of the off-midline tongue base (arrows). CT scan at the level of the lower neck failed to disclose normal thyroid tissue in the thyroid bed at the anterior aspect of the thyroid cartilage (not shown). B. Anteroposterior 131I scan shows round hot uptake at the center of the oropharynx, and this matches the location of the lesion revealed by CT (arrow). No uptake is seen in the normal thyroid bed indicated by isotope markers (open arrows). CT and scintigraphy can thus be used to diagnose lingual thyroid. No treatment was undertaken.
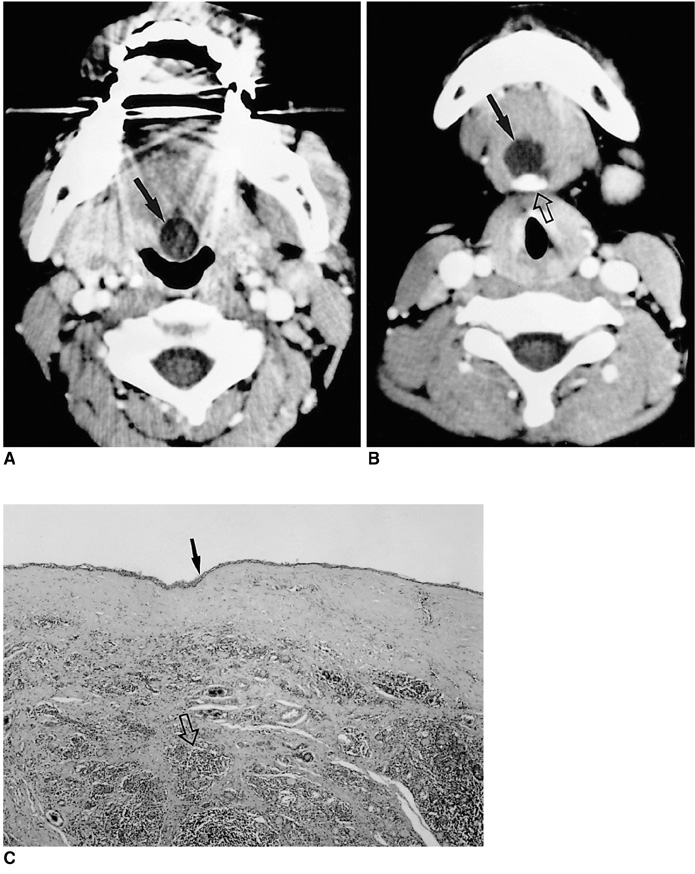
Fig. 2 Lingual thyroglossal duct cyst in a 2-year-old boy with stridor and dysphagia. A. Contrast-enhanced axial CT scan shows a well-demarcated cyst in the region of the foramen cecum at the base of the tongue (arrow). B. Axial CT scan 1.5cm caudal to A shows downward extension of the cyst to the level of the hyoid bone (open arrow) along the tract of the thyroglossal duct. C. Photomicrograph (original magnification ×40; H & E staining) demonstrates remnant thyroid tissue (open arrow) and inflammatory cells, suggesting complication, lined by cuboidal to columnar epithelium (arrow).

Fig. 3 Bronchogenic cyst in a 19-year-old man with macroglossia since infancy. A. Contrast-enhanced CT scan shows a large, lobulated, thin-walled cystic mass at the central portion of the tongue (black arrow). Note the submucosal location of this mass and the intact overlying mucosa (white arrow). The mass demonstrates homogeneous low attenuation but a high-attenuated solid component at the posterior aspect suggests mucin content (open arrow). The differential diagnosis included dermoid cyst and lymphangioma. B. Photomicrograph (original magnification ×200; H & E staining) shows that the cyst is lined by ciliated pseudostratified epithelium of the respiratory type (arrows) and contains a small amount of mucin secretion (arrowheads).
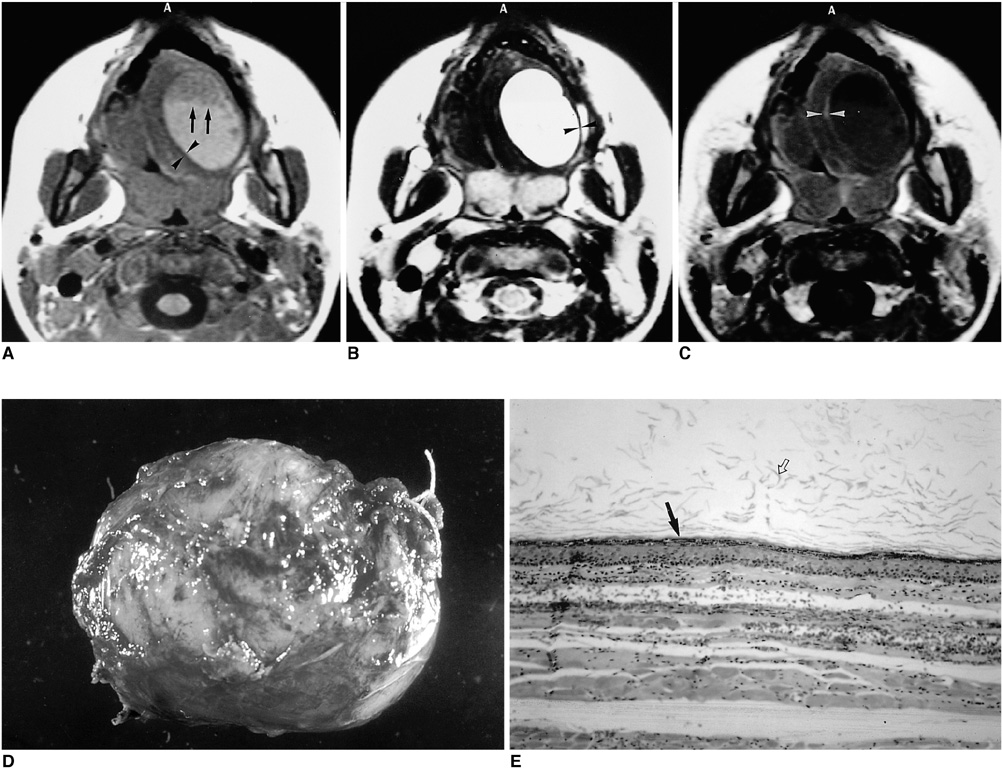
Fig. 4 Epidermoid cyst in a 5-year-old boy with bulging mass of the tongue since infancy. A. T1-weighted axial image shows a large, unilocular cystic lesion with a fluid-fluid level (arrows) surrounded by a thin low signal rim (arrowheads) at the left lateral aspect of the tongue. B. T2-weighted axial image demonstrates the high signal intensity of the lesion and a surrounding, thin, low signal rim that may represent either adjacent compressed tissue or a capsule (arrowheads). C. Enhanced T1-weighted axial image reveals enhancement of the peripheral rim only (arrowheads). D. Photograph of a gross specimen shows a well-defined, thin-walled cystic mass. E. Photomicrograph (original magnification ( 100; H & E staining) indicates that the cyst is covered with simple squamous cell epithelium (arrow), has a fibrous wall and atrophic muscle, and contains keratinaceous materials (open arrow).
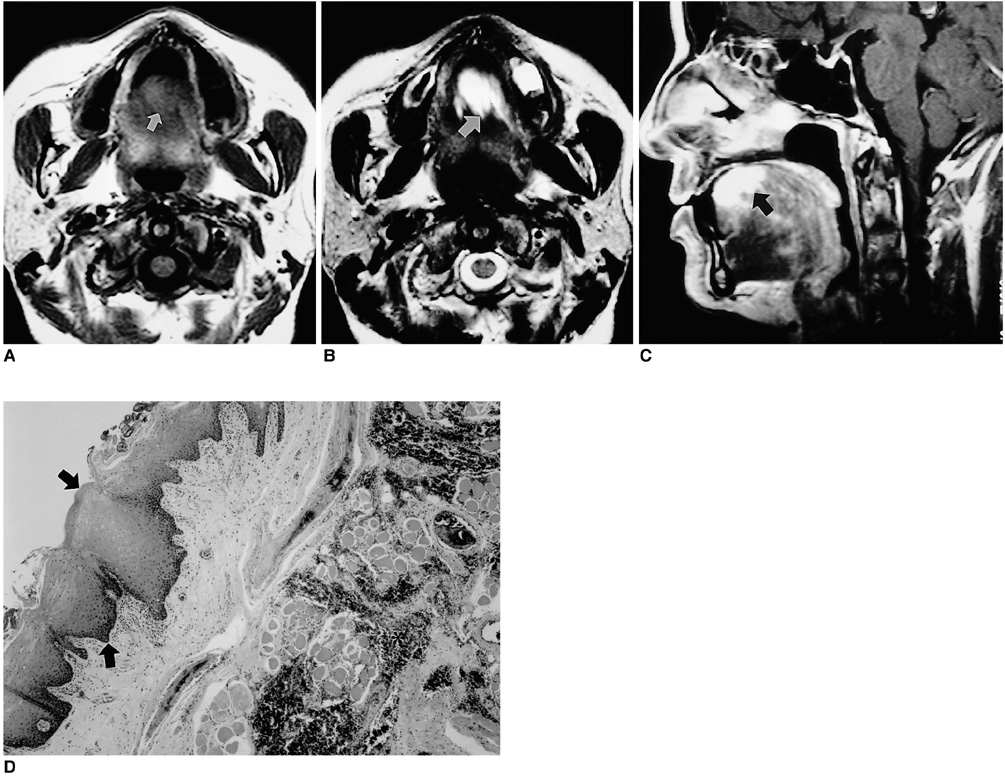
Fig. 5 Venous malformation in a 35-year-old female with a bluish tongue mass. A. T1-weighted axial image shows a mass with slightly high signal intensity (arrow) at the anterior portion of the tongue. B. T2-weighted axial image shows a lesion with high signal intensity (arrow). C. Enhanced T1-weighted sagittal image demonstrates strong enhancement of the lesion (arrow). D. Photomicrograph (original magnification ×40; H & E staining) shows a poorly defined venous malformation covered with stratified squamous epithelium (arrows). Note the presence of large, markedly dilated vascular spaces (*) lined by endothelium and communicating with each other.
Cited by 1 articles
-
Congenital Epidermoid Cyst of the Oral Cavity: Prenatal Diagnosis by Sonography
Seung Wan Park, Jung Ju Lee, Soo Ahn Chae, Byoung Hoon Yoo, Gwang Jun Kim, Sei Young Lee
Clin Exp Otorhinolaryngol. 2013;6(3):191-193. doi: 10.3342/ceo.2013.6.3.191.
Reference
-
1. Sauk JJ Jr. Ectopic lingual thyroid. J Pathol. 1970. 102:239–243.2. Shah HR, Boyd CM, Williamson M, et al. Lingual thyroid: unusual appearance on computed tomography. Comput Med Imaging Graph. 1988. 12:263–266.3. Santiago W, Rybak LP, Bass RM. Thyroglossal duct cyst of the tongue. J Otolaryngol. 1985. 14:261–264.4. Vogl TJ, Steger W, Ihrler S, Ferrera P, Grevers G. Cystic masses in the floor of the mouth: value of MR imaging in planning surgery. AJR. 1993. 161:183–186.5. Dee P. Armstrong P, Wilson AG, Hansell DM, editors. Congenital disorders of the lungs and airways. Imaging of diseases of the chest. 1995. 2nd ed. St. Louis: Mosby Year Book;610–614.6. Meyer I. Dermoid cysts (dermoids) of the floor of the mouth. Oral Surg Oral Med Oral Pathol. 1955. 8:1149–1164.7. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982. 69:412–420.8. Fishman SJ, Mulliken JB. Hemangiomas and vascular malformations of infancy and childhood. Pediatr Clin North Am. 1993. 40:1177–1200.9. Burrows PE, Mulliken JB, Fellows KE, Strand RD. Childhood hemangiomas and vascular malformations: angiographic differentiation. AJR. 1983. 141:483–488.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiologic-Pathologic Correlation of Unusual Lingual Masses:Part II: Benign and Malignant Tumors
- Recurrent Bronchiolitis in an Infant: An Unusual Presentation of Lingual Thyroglossal Duct Cyst
- Macrodystrophia lipomatosa
- Cystic Lesions of the Gastrointestinal Tract: Multimodality Imaging with Pathologic Correlations
- Unusual Primary Subepithelial Tumors of the Colon: Multimodality Imaging Findings with Endoscopic and Pathologic Correlation
