Cystic Lesions of the Gastrointestinal Tract: Multimodality Imaging with Pathologic Correlations
- Affiliations
-
- 1Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Seoul 152-703, Korea. jongmee.lee@gmail.com
- 2Department of Pathology, Korea University Guro Hospital, Korea University College of Medicine, Seoul 152-703, Korea.
- 3Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- 4Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 135-710, Korea.
- KMID: 984900
- DOI: http://doi.org/10.3348/kjr.2010.11.4.457
Abstract
- The cystic lesions of the gastrointestinal (GI) tract demonstrate the various pathologic findings. Some lesions may present a diagnostic challenge because of non-specific imaging features; however, other lesions are easily diagnosed using characteristic radiologic features and anatomic locations. Cystic masses from the GI tract can be divided into several categories: congenital lesions, neoplastic lesions (cystic neoplasms, cystic degeneration of solid neoplasms), and other miscellaneous lesions. In this pictorial review, we describe the pathologic findings of various cystic lesions of the GI tract as well as the radiologic features of GI cystic lesions from several imaging modalities including a barium study, transabdominal ultrasound (US), computed tomography (CT), and magnetic resonance (MR) imaging.
Keyword
MeSH Terms
Figure
-
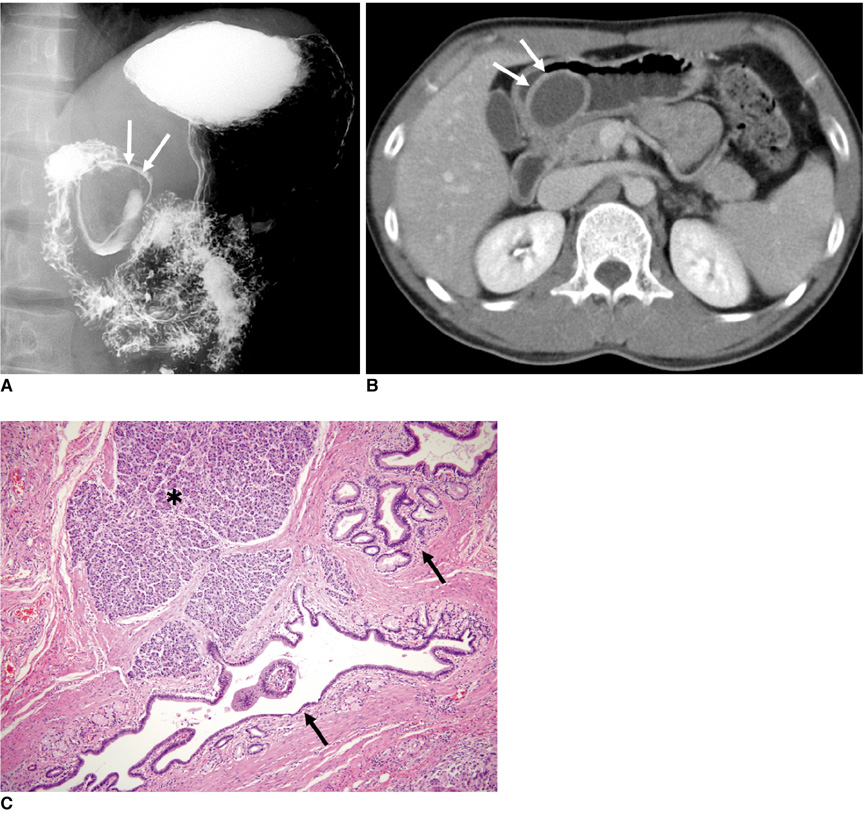
Fig. 1 Gastric duplication cyst in 29-year-old man. A. Upper gastrointestinal series shows oval polypoid mass (arrows) with smooth border in gastric antrum. B. Contrast-enhanced CT scan demonstrates oval cystic lesion with evenly enhancing wall (arrows) in posterior wall of gastric antrum. C. Photomicrograph demonstrates normal gastric mucosa (arrows) and smooth muscle layer. Heterotopic pancreatic tissue island (asterisk) is shown in submucosal layer (Hematoxylin & Eosin stain, ×100).
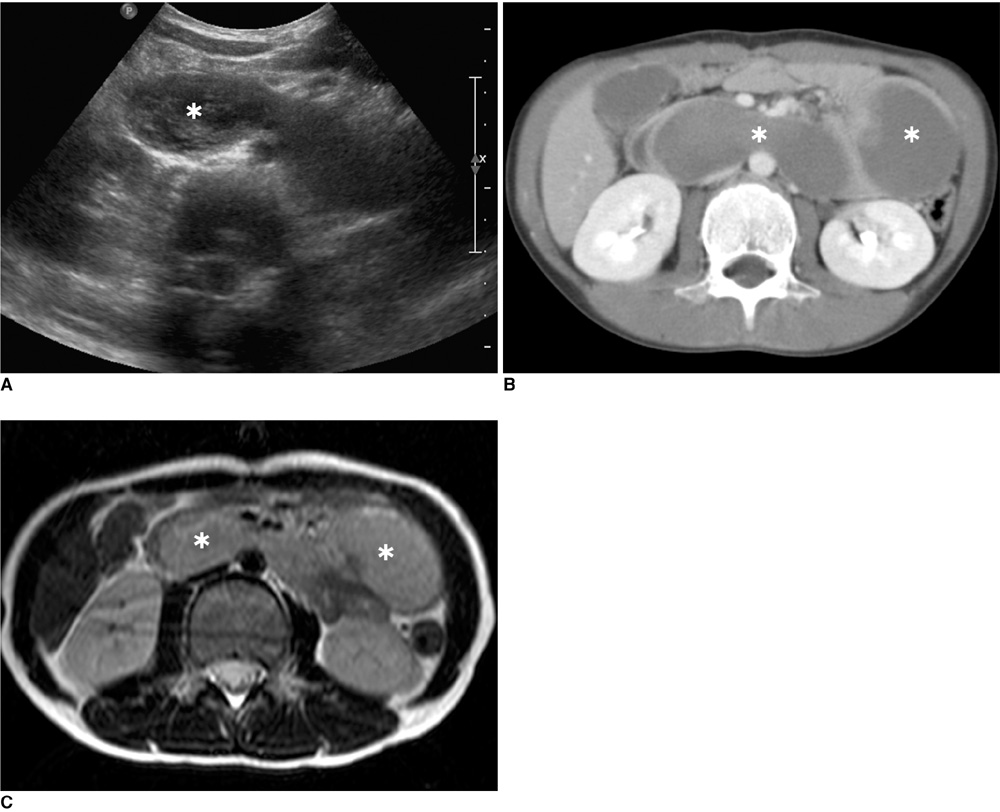
Fig. 2 Duodenal duplication cyst in 9-year-old boy. A. Transabdominal ultrasound shows tubular cystic lesion with internal debris (asterisk) in anterior aspect of both kidneys. B. CT scan demonstrates tubular cystic lesion (asterisks) along duodenum and extending toward jejunum. Cystic lesion showed presence of fluid with higher attenuation than water, suggestive of hemorrhage on precontrast CT scan (not shown). C. T2-weighted MR imaging shows well-circumscribed mass (asterisks) with slightly high signal intensity in abdomen.
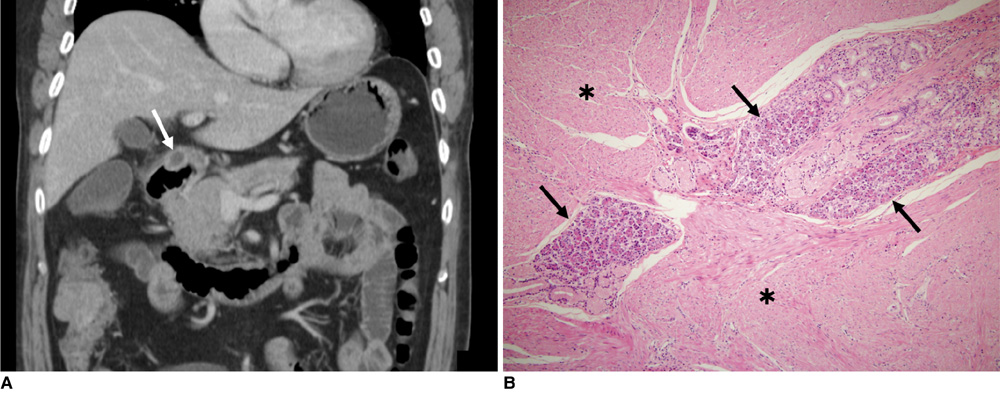
Fig. 3 Heterotopic pancreas in 57-year-old man with cecal cancer. A. Contrast-enhanced CT scan shows small cystic lesion (arrow) in gastric antrum. B. Photomicrograph shows heterotopic pancreatic acini islands (arrows) in smooth muscle layer of stomach (asterisks; Hematoxylin & Eosin stain, ×100).
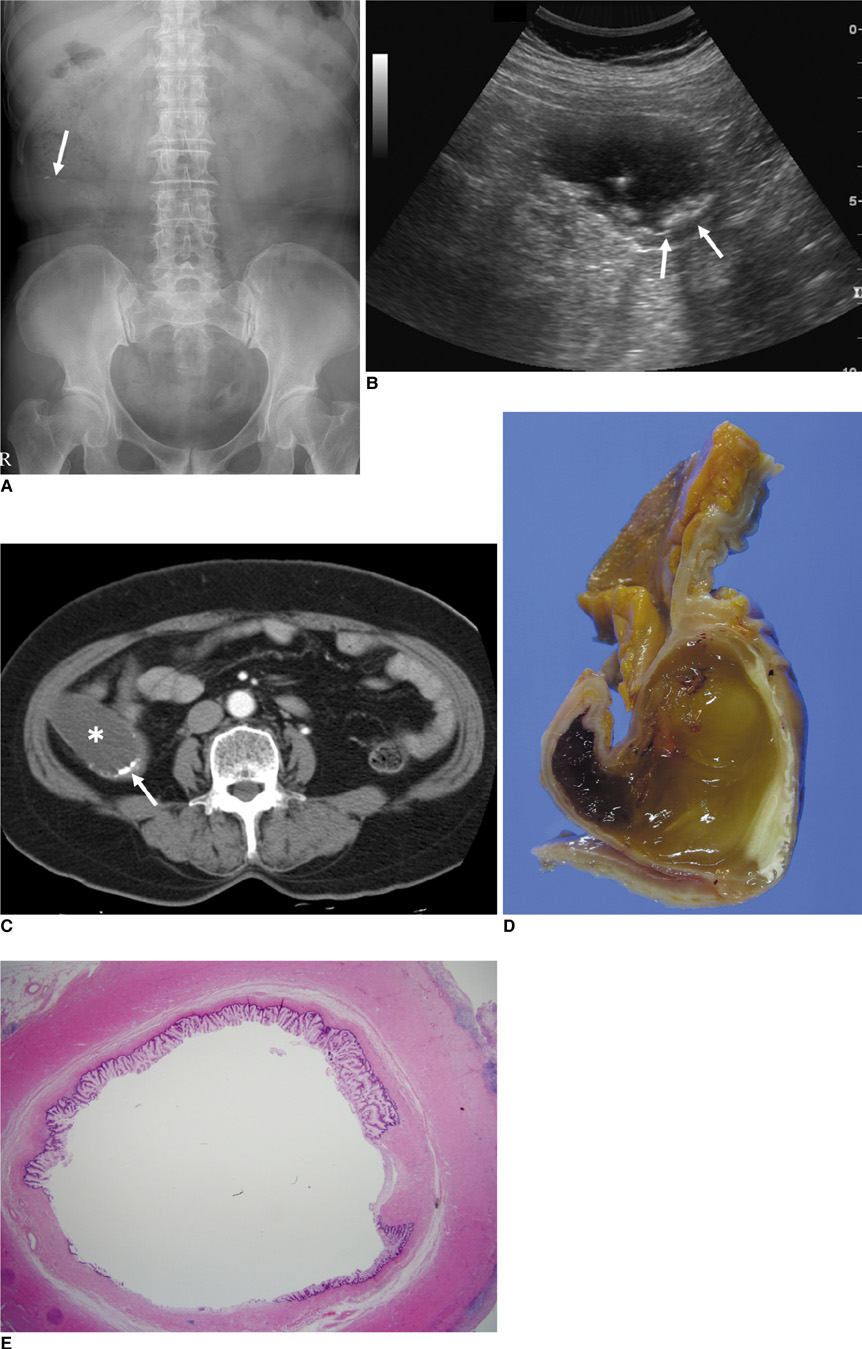
Fig. 4 Mucinous cystadenoma of appendix in 67-year-old man. A. Plain abdominal radiograph shows curvilinear calcifications (arrow) in right lower abdomen. B. Transabdominal ultrasound demonstrates elongated cystic mass in appendiceal area. There are small echogenic lesions with posterior acoustic shadowing (arrows) along wall of appendix. C. Contrast-enhanced CT scan shows tubular dilatation of appendix with fluid attenuation (asterisk) and some wall calcifications (arrow). D. Cross-section of appendix demonstrates that appendiceal lumen is completely filled with gelatinous mucoid material. E. Photomicrograph shows villiform mucin-secreting epithelium lining appendiceal lumen (Hematoxylin & Eosin stain, ×12.5).
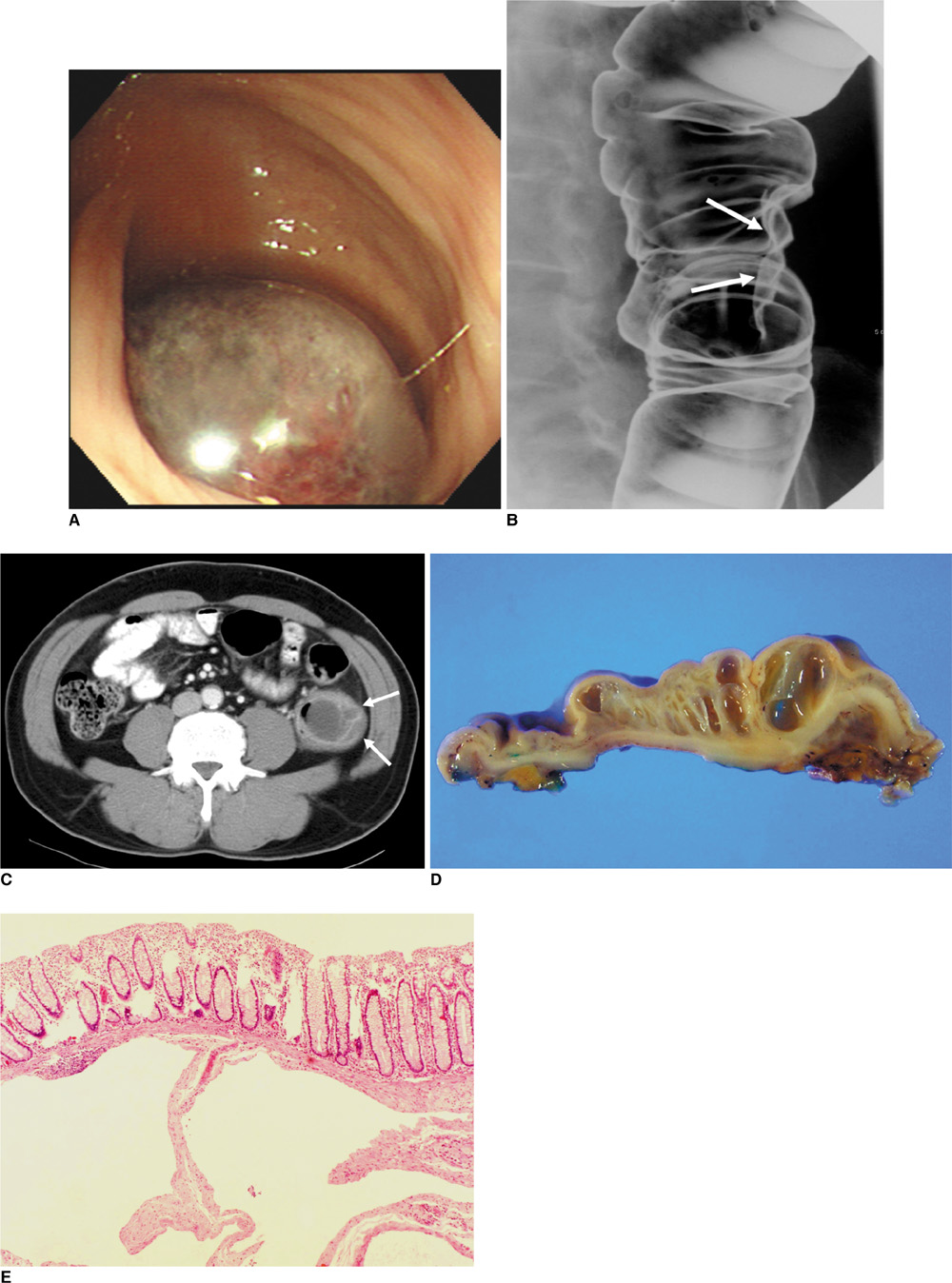
Fig. 5 Cystic lymphangioma in colon of 57-year-old man. A. Endoscopy shows blue-tinged, submucosal mass with smooth surface in descending colon. B. Barium study demonstrates smooth-surfaced polypoid mass (arrows) in lateral wall of descending colon. C. Contrast-enhanced CT scan shows multiseptate cystic mass (arrows) in descending colon. D. Cut surface of gross specimen reveals septated cystic mass with clear fluid in submucosal layer of descending colon. E. Photomicrograph shows variable-sized, thin-walled cystic spaces lined with flattened endothelial cells (Hematoxylin & Eosin stain, ×40).
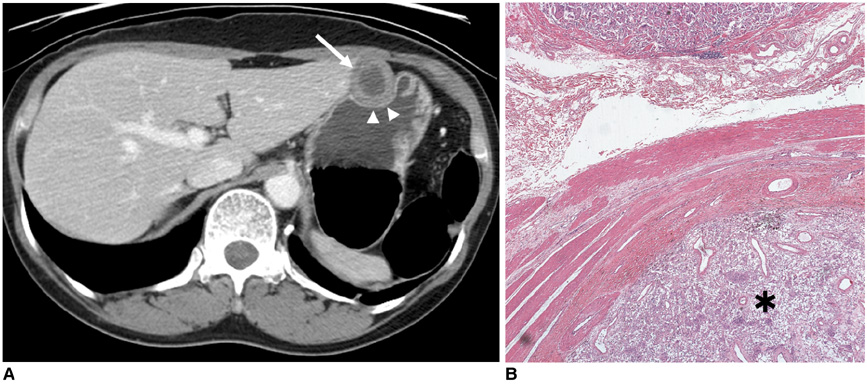
Fig. 6 Gastric gastrointestinal stromal tumor with cystic changes in 58-year-old woman. A. Contrast-enhanced CT scan shows well-defined cystic mass (arrow) in anterior wall of gastric body. Mass appears to have homogeneous low attenuation with thick, enhancing rim. Note intact overlying gastric mucosa (arrowheads). B. Photomicrograph shows mass composed of spindle cells (asterisk) in muscular layer of stomach (Hematoxylin & Eosin stain, ×40).
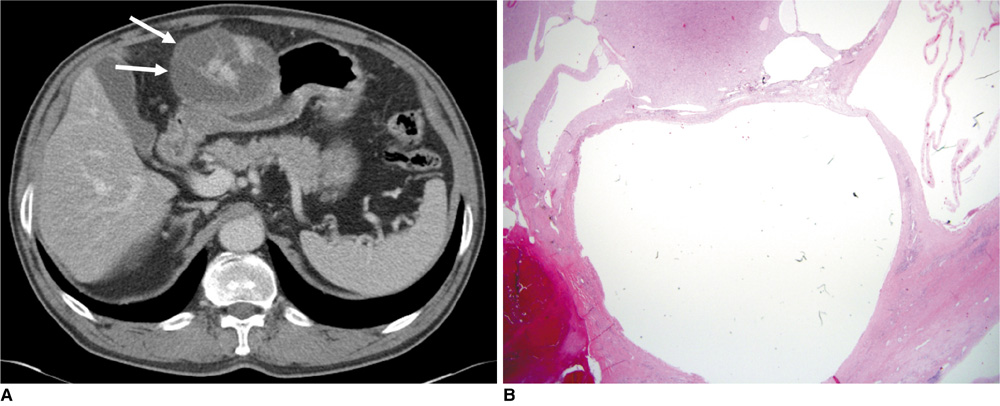
Fig. 7 Gastric gastrointestinal stromal tumor with hemorrhage in 71-year-old man. A. Contrast-enhanced CT scan shows multilocular cystic mass (arrows) in anterior wall of gastric antrum. B. Photomicrograph shows multiple large cystic spaces in mass composed of spindle cells (Hematoxylin & Eosin stain, ×12.5).

Fig. 8 Gastric schwannoma with cystic changes in 58-year-old woman. A. Contrast-enhanced CT scan shows well-defined cystic mass (arrow) abutting anterior wall of gastric antrum. B. Cut surface of surgical specimen of stomach shows cystic change (arrow) in central portion of mass. C. Photomicrograph shows highly cellular area composed of spindle cells and loose meshwork (asterisk). Note peripheral lymphoid cuffs (arrows; Hematoxylin & Eosin stain, ×40).
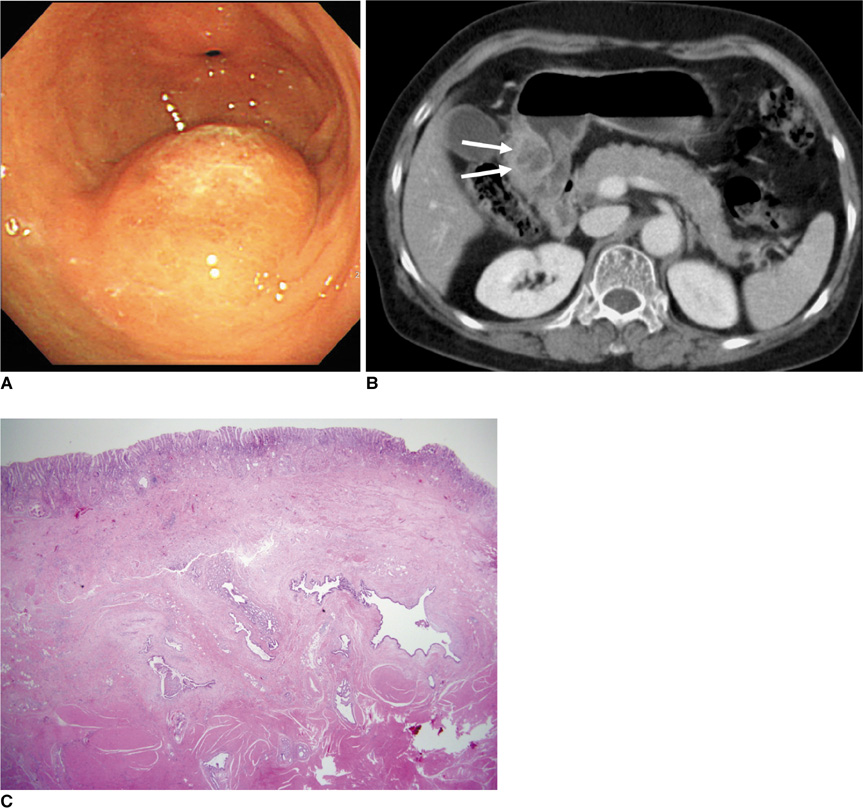
Fig. 9 Gastritis cystica profunda in 61-year-old woman. A. Endoscopy shows polypoid lesion with smooth surface and patches of erythema, but no erosions. Surrounding mucosa appears normal. B. Contrast-enhanced CT scan shows polypoid cystic mass in gastric antrum (arrows). C. Photomicrograph shows cystic dilatation of heterotopic gastric glands in submucosal and muscular layers (Hematoxylin & Eosin stain, ×12.5).
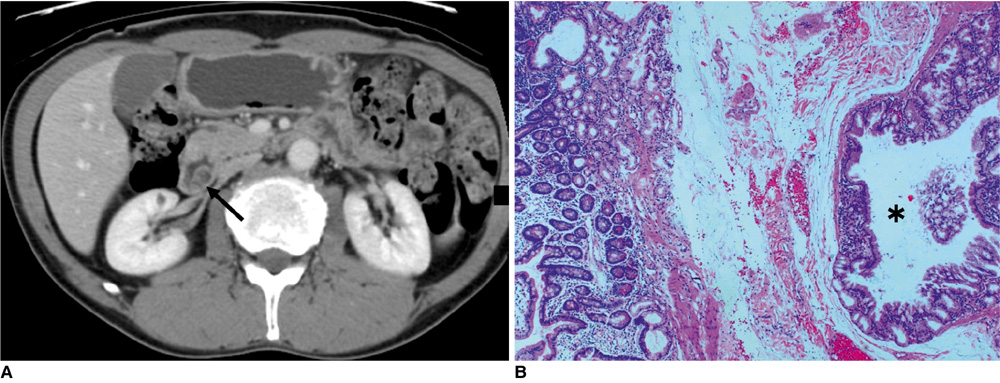
Fig. 10 Brunner's gland hyperplasia in 48-year-old man. A. Contrast-enhanced CT scan shows cystic mass (arrow) in second section of duodenum. B. Photomicrograph demonstrates cystic changes of hyperplastic Brunner's glands (asterisk) with lobular architecture in submucosa (Hematoxylin & Eosin stain, ×40).
Reference
-
1. Macpherson RI. Gastrointestinal tract duplications: clinical, pathologic, etiologic, and radiologic considerations. Radiographics. 1993. 13:1063–1080.2. Bower RJ, Sieber WK, Kiesewetter WB. Alimentary tract duplications in children. Ann Surg. 1978. 188:669–674.3. Theodosopoulos T, Marinis A, Karapanos K, Vassilikostas G, Dafnios N, Samanides L, et al. Foregut duplication cysts of the stomach with respiratory epithelium. World J Gastroenterol. 2007. 13:1279–1281.4. Kangarloo H, Sample WF, Hansen G, Robinson JS, Sarti D. Ultrasonic evaluation of abdominal gastrointestinal tract duplication in children. Radiology. 1979. 131:191–194.5. Wang C, Kuo Y, Yeung K, Wu C, Liu G. CT appearance of ectopic pancreas: a case report. Abdom Imaging. 1998. 23:332–333.6. Levine MS. Gore RM, Levine MS, editors. Benign tumors of the stomach and duodenum. Textbook of gastrointestinal radiology. 2008. 3rd ed. Philadelphia, PA: Saunders Elsevier;593–617.7. Cho JS, Shin KS, Kwon ST, Kim JW, Song CJ, Noh SM, et al. Heterotopic pancreas in the stomach: CT findings. Radiology. 2000. 217:139–144.8. Lopez-Pelaez MS, Hoyos FB, Isidro MG, Unzurrunzaga EA, Lopez Ede V, Collazo YQ. Cystic dystrophy of heterotopic pancreas in stomach: radiologic and pathologic correlation. Abdom Imaging. 2008. 33:391–394.9. Park SH, Han JK, Choi BI, Kim M, Kim YI, Yeon KM, et al. Heterotopic pancreas of the stomach: CT findings correlated with pathologic findings in six patients. Abdom Imaging. 2000. 25:119–123.10. Dachman AH, Lichtenstein JE, Friedman AC. Mucocele of the appendix and pseudomyxoma peritonei. AJR Am J Roentgenol. 1985. 144:923–929.11. Fenoglio-Preiser CM. Gastrointestinal pathology: an atlas and text. 2008. 3rd ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins.12. Pickhardt PJ, Levy AD, Rohrmann CA Jr, Kende AI. Primary neoplasms of the appendix: radiologic spectrum of disease with pathologic correlation. Radiographics. 2003. 23:645–662.13. Sasaki K, Ishida H, Komatsuda T, Suzuki T, Konno K, Ohtaka M, et al. Appendiceal mucocele: sonographic findings. Abdom Imaging. 2003. 28:15–18.14. Zhu H, Wu ZY, Lin XZ, Shi B, Upadhyaya M, Chen K. Gastrointestinal tract lymphangiomas: findings at CT and endoscopic imaging with histopathologic correlation. Abdom Imaging. 2008. 33:662–668.15. Agha FP, Francis IR, Simms SM. Cystic lymphangioma of the colon. AJR Am J Roentgenol. 1983. 141:709–710.16. Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, et al. Diagnosis of gastrointestinal stromal tumors: a consensus approach. Hum Pathol. 2002. 33:459–465.17. Levy AD, Remotti HE, Thompson WM, Sobin LH, Miettinen M. Gastrointestinal stromal tumors: radiologic features with pathologic correlation. Radiographics. 2003. 23:283–304.18. Levy AD, Quiles AM, Miettinen M, Sobin LH. Gastrointestinal schwannomas: CT features with clinicopathologic correlation. AJR Am J Roentgenol. 2005. 184:797–802.19. Hou YY, Tan YS, Xu JF, Wang XN, Lu SH, Ji Y, et al. Schwannoma of the gastrointestinal tract: a clinicopathological, immunohistochemical and ultrastructural study of 33 cases. Histopathology. 2006. 48:536–545.20. Miettinen M, Shekitka KM, Sobin LH. Schwannomas in the colon and rectum: a clinicopathologic and immunohistochemical study of 20 cases. Am J Surg Pathol. 2001. 25:846–855.21. Fujii Y, Taniguchi N, Hosoya Y, Yoshizawa K, Yasuda Y, Nagai H, et al. Gastric schwannoma: sonographic findings. J Ultrasound Med. 2004. 23:1527–1530.22. Franzin G, Novelli P. Gastritis cystica profunda. Histopathology. 1981. 5:535–547.23. Kurland J, DuBois S, Behling C, Savides T. Severe upper-GI bleed caused by gastritis cystica profunda. Gastrointest Endosc. 2006. 63:716–717.24. Wu MT, Pan HB, Lai PH, Chang JM, Tsai SH, Wu CW. CT of gastritis cystica polyposa. Abdom Imaging. 1994. 19:8–10.25. Giacosa A. Morphometry of normal duodenal mucosa. Scand J Gastroenterol Suppl. 1989. 167:10–12.26. Levine MS. Gore RM, Levine MS, editors. Benign tumors of the stomach and duodenum. Textbook of gastrointestinal radiology. 2008. 3rd ed. Philadelphia, PA: Saunders Elsevier;593–617.27. Patel ND, Levy AD, Mehrotra AK, Sobin LH. Brunner's gland hyperplasia and hamartoma: imaging features with clinicopathologic correlation. AJR Am J Roentgenol. 2006. 187:715–722.28. Stolpman DR, Hunt GC, Sheppard B, Huang H, Gopal DV. Brunner's gland hamartoma: a rare cause of gastrointestinal bleeding - case report and review of the literature. Can J Gastroenterol. 2002. 16:309–313.29. Block KP, Frick TJ, Warner TF. Gastrointestinal bleeding from a Brunner's gland hamartoma: characterization by endoscopy, computed tomography, and endoscopic ultrasound. Am J Gastroenterol. 2000. 95:1581–1583.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perirectal Cystic Lesions - Comprehensive CT and MRI Findings
- The Diagnosis of Subepithelial Lesions in the Upper Gastrointestinal Tract
- Pathologic Features of Pancreatic Cystic Neoplasms
- Diagnostic Value of ERCP in Pancreatic Cystic Lesions
- Role of linked color imaging for upper gastrointestinal disease: present and future
