Kosin Med J.
2023 Dec;38(4):241-251. 10.7180/kmj.23.151.
Basic knowledge of endoscopic retrograde cholangiopancreatography
- Affiliations
-
- 1Department of Internal Medicine, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan, Korea
- KMID: 2549496
- DOI: http://doi.org/10.7180/kmj.23.151
Abstract
- Endoscopic retrograde cholangiopancreatography (ERCP) was first performed in the late 1960s. Due to advancements in instruments, devices, and techniques, ERCP has played an important role in the management and diagnosis of pancreatobiliary disorders. However, ERCP is accompanied by the risk of various complications even if performed by an expert. The incidence of ERCP complications is approximately 4% to 10%, while the incidence of fatal complications, such as death, is less than 0.5%. To prevent adverse events, experts performing ERCP must recognize and address ERCP-related complications and understand the various techniques. In this review, we summarize the complications and techniques of ERCP.
Figure
-

Fig. 1. An incision below the transverse fold was classified as a small incision; an incision up to the superior margin of the papillary bulge was a large incision; and an incision in the middle, as a medium incision.

Fig. 2. When a guidewire is cannulated in the main pancreatic duct during a selective cannulation attempt, selective biliary cannulation using another guidewire without removing the first guidewire is called the double-guidewire technique.

Fig. 3. Pushing the endoscope along the gastric greater curvature.
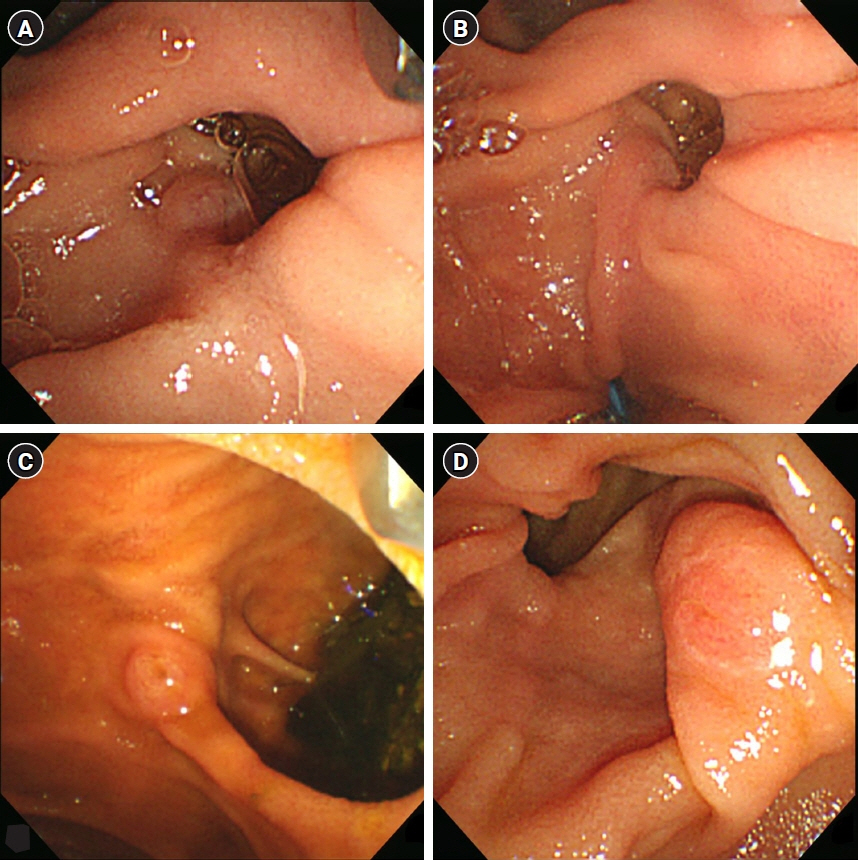
Fig. 4. Periampullary diverticulum types. (A) Type 1, (B) type 1, (C) type 2, (D) type 3.
Reference
-
References
1. Kang G, Kim SE. How to write an original article in medicine and medical science. Kosin Med J. 2022; 37:96–101.2. Kim DJ, Kil SY, Son J, Lee HS. How to conduct well-designed clinical research. Kosin Med J. 2022; 37:187–91.3. Lee HS. Ethical issues in clinical research and publication. Kosin Med J. 2022; 37:278–82.4. American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointest Endosc. 2000; 52:831–7.5. ASGE Technology Committee, Kethu SR, Adler DG, Conway JD, Diehl DL, Farraye FA, et al. ERCP cannulation and sphincterotomy devices. Gastrointest Endosc. 2010; 71:435–45.6. Laasch HU, Tringali A, Wilbraham L, Marriott A, England RE, Mutignani M, et al. Comparison of standard and steerable catheters for bile duct cannulation in ERCP. Endoscopy. 2003; 35:669–74.7. Clayton ES, Connor S, Alexakis N, Leandros E. Meta-analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. Br J Surg. 2006; 93:1185–91.8. Dumonceau JM, Kapral C, Aabakken L, Papanikolaou IS, Tringali A, Vanbiervliet G, et al. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2020; 52:127–49.9. Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996; 335:909–19.10. Hamada T, Yasunaga H, Nakai Y, Isayama H, Matsui H, Horiguchi H, et al. Bleeding after endoscopic sphincterotomy or papillary balloon dilation among users of antithrombotic agents. Endoscopy. 2015; 47:997–1004.11. Kim KO, Kim TN, Kim SB, Lee JY. Characteristics of delayed hemorrhage after endoscopic sphincterotomy. J Gastroenterol Hepatol. 2010; 25:532–8.12. Verma D, Kapadia A, Adler DG. Pure versus mixed electrosurgical current for endoscopic biliary sphincterotomy: a meta-analysis of adverse outcomes. Gastrointest Endosc. 2007; 66:283–90.13. Mirjalili SA, Stringer MD. The arterial supply of the major duodenal papilla and its relevance to endoscopic sphincterotomy. Endoscopy. 2011; 43:307–11.14. Petersen BT, Hussain N, Marine JE, Trohman RG, Carpenter S, Chuttani R, et al. Endoscopy in patients with implanted electronic devices. Gastrointest Endosc. 2007; 65:561–8.15. Tse F, Yuan Y. Early routine endoscopic retrograde cholangiopancreatography strategy versus early conservative management strategy in acute gallstone pancreatitis. Cochrane Database Syst Rev. 2012; (5):CD009779.16. Lehman GA. What are the determinants of success in utilization of ERCP in the setting of pancreatic and biliary diseases? Gastrointest Endosc. 2002; 56(6 Suppl):S291–3.17. Freeman ML, Guda NM. ERCP cannulation: a review of reported techniques. Gastrointest Endosc. 2005; 61:112–25.18. Yasuda I, Isayama H, Bhatia V. Current situation of endoscopic biliary cannulation and salvage techniques for difficult cases: current strategies in Japan. Dig Endosc. 2016; 28 Suppl 1:62–9.19. Dhir V, Bhandari S, Bapat M, Maydeo A. Comparison of EUS-guided rendezvous and precut papillotomy techniques for biliary access (with videos). Gastrointest Endosc. 2012; 75:354–9.20. Isayama H, Nakai Y, Koike K. Is a guidewire a magic wand? Is a knife the final weapon? Saudi J Gastroenterol. 2015; 21:3–4.21. Bove V, Tringali A, Familiari P, Gigante G, Boskoski I, Perri V, et al. ERCP in patients with prior Billroth II gastrectomy: report of 30 years’ experience. Endoscopy. 2015; 47:611–6.22. Shimatani M, Matsushita M, Takaoka M, Koyabu M, Ikeura T, Kato K, et al. Effective “short” double-balloon enteroscope for diagnostic and therapeutic ERCP in patients with altered gastrointestinal anatomy: a large case series. Endoscopy. 2009; 41:849–54.23. Kim MH, Lee SK, Lee MH, Myung SJ, Yoo BM, Seo DW, et al. Endoscopic retrograde cholangiopancreatography and needle-knife sphincterotomy in patients with Billroth II gastrectomy: a comparative study of the forward-viewing endoscope and the side-viewing duodenoscope. Endoscopy. 1997; 29:82–5.24. Hintze RE, Veltzke W, Adler A, Abou-Rebyeh H. Endoscopic sphincterotomy using an S-shaped sphincterotome in patients with a Billroth II or Roux-en-Y gastrojejunostomy. Endoscopy. 1997; 29:74–8.25. Bergman JJ, van Berkel AM, Bruno MJ, Fockens P, Rauws EA, Tijssen JG, et al. A randomized trial of endoscopic balloon dilation and endoscopic sphincterotomy for removal of bile duct stones in patients with a prior Billroth II gastrectomy. Gastrointest Endosc. 2001; 53:19–26.26. Zoepf T, Zoepf DS, Arnold JC, Benz C, Riemann JF. The relationship between juxtapapillary duodenal diverticula and disorders of the biliopancreatic system: analysis of 350 patients. Gastrointest Endosc. 2001; 54:56–61.27. Fujita N, Noda Y, Kobayashi G, Kimura K, Yago A. ERCP for intradiverticular papilla: two-devices-in-one-channel method: endoscopic retrograde cholangiopancreatography. Gastrointest Endosc. 1998; 48:517–20.28. Scotiniotis I, Ginsberg GG. Endoscopic clip-assisted biliary cannulation: externalization and fixation of the major papilla from within a duodenal diverticulum using the endoscopic clip fixing device. Gastrointest Endosc. 1999; 50:431–3.29. Ding X, Zhang F, Wang Y. Risk factors for post-ERCP pancreatitis: a systematic review and meta-analysis. Surgeon. 2015; 13:218–29.30. El Nakeeb A, El Hanafy E, Salah T, Atef E, Hamed H, Sultan AM, et al. Post-endoscopic retrograde cholangiopancreatography pancreatitis: risk factors and predictors of severity. World J Gastrointest Endosc. 2016; 8:709–15.31. Njei B, Sharma P, McCarty TR, Singh M, Haque L, Aslanian HR, et al. Cannabis use is associated with increased risk of post-endoscopic retrograde cholangiopancreatography pancreatitis: analysis of the US nationwide inpatient sample database, 2004-2014. Pancreas. 2018; 47:1142–9.32. Freeman ML, Guda NM. Prevention of post-ERCP pancreatitis: a comprehensive review. Gastrointest Endosc. 2004; 59:845–64.33. Luo H, Zhao L, Leung J, Zhang R, Liu Z, Wang X, et al. Routine pre-procedural rectal indometacin versus selective post-procedural rectal indometacin to prevent pancreatitis in patients undergoing endoscopic retrograde cholangiopancreatography: a multicentre, single-blinded, randomised controlled trial. Lancet. 2016; 387:2293–301.34. Patai A, Solymosi N, Patai AV. Does rectal indomethacin given for prevention of post-ERCP pancreatitis increase bleeding after biliary endoscopic sphincterotomy or cardiovascular mortality? Post hoc analysis using prospective clinical trial data. Medicine (Baltimore). 2014; 93:e159.35. Barthet M, Lesavre N, Desjeux A, Gasmi M, Berthezene P, Berdah S, et al. Complications of endoscopic sphincterotomy: results from a single tertiary referral center. Endoscopy. 2002; 34:991–7.36. Ferreira LE, Baron TH. Post-sphincterotomy bleeding: who, what, when, and how. Am J Gastroenterol. 2007; 102:2850–8.37. Wilcox CM, Canakis J, Monkemuller KE, Bondora AW, Geels W. Patterns of bleeding after endoscopic sphincterotomy, the subsequent risk of bleeding, and the role of epinephrine injection. Am J Gastroenterol. 2004; 99:244–8.38. Kuran S, Parlak E, Oguz D, Cicek B, Disibeyaz S, Sahin B. Endoscopic sphincterotomy-induced hemorrhage: treatment with heat probe. Gastrointest Endosc. 2006; 63:506–11.39. Takano S, Fukasawa M, Shindo H, Takahashi E, Hirose S, Fukasawa Y, et al. Risk factors for perforation during endoscopic retrograde cholangiopancreatography in post-reconstruction intestinal tract. World J Clin Cases. 2019; 7:10–8.40. Fatima J, Baron TH, Topazian MD, Houghton SG, Iqbal CW, Ott BJ, et al. Pancreaticobiliary and duodenal perforations after periampullary endoscopic procedures: diagnosis and management. Arch Surg. 2007; 142:448–55.41. Weinberg BM, Shindy W, Lo S. Cochrane Database Syst Rev. Arch Surg. 2006; 2006:CD004890.42. Feng Y, Zhu H, Chen X, Xu S, Cheng W, Ni J, et al. Comparison of endoscopic papillary large balloon dilation and endoscopic sphincterotomy for retrieval of choledocholithiasis: a meta-analysis of randomized controlled trials. J Gastroenterol. 2012; 47:655–63.43. Fujimoto T, Tsuyuguchi T, Sakai Y, Sugiyama H, Miyakawa K, Eto R, et al. Long-term outcome of endoscopic papillotomy for choledocholithiasis with cholecystolithiasis. Dig Endosc. 2010; 22:95–100.44. Park BK, Seo JH, Jeon HH, Choi JW, Won SY, Cho YS, et al. A nationwide population-based study of common bile duct stone recurrence after endoscopic stone removal in Korea. J Gastroenterol. 2018; 53:670–8.45. Khan MA, Khan Z, Tombazzi CR, Gadiparthi C, Lee W, Wilcox CM. Role of cholecystectomy after endoscopic sphincterotomy in the management of choledocholithiasis in high-risk patients: a systematic review and meta-analysis. J Clin Gastroenterol. 2018; 52:579–89.46. Chen M, Wang L, Wang Y, Wei W, Yao YL, Ling TS, et al. Risk factor analysis of post-ERCP cholangitis: a single-center experience. Hepatobiliary Pancreat Dis Int. 2018; 17:55–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Training in Endoscopy: Endoscopic Retrograde Cholangiopancreatography
- Is Endoscopic Retrograde Cholangiopancreatography Essential for Assessment of Traumatic Pancreas Injury?
- Endoscopic Retrograde Cholangiopancreatography in Post Gastrectomy Patients
- The Management of Endoscopic Retrograde Cholangiopancreatography-Related Duodenal Perforation
- Can Endoscopic Ultrasonography Prevent Unnecessary Endoscopic Retrograde Cholangiopancreatography in Patients with High and Intermediate Likelihood of Choledocholithiasis?
