Distally-extending muscle fibers across involved joints: study of long muscles and tendons of wrist and ankle in late-term fetuses and adult cadavers
- Affiliations
-
- 1Department of Anatomy, Wuxi School of Medicine, Jiangnan University, Wuxi, China
- 2Department of Anatomy, Division of Basic Medicine, Tokai University School of Medicine, Isehara, Kanagawa, Japan
- 3Department of Anatomy, Chonbuk National University Medical School, Jeonju, Korea
- 4Department of Anatomy, Tokyo Dental College, Tokyo, Japan
- 5Division of Internal Medicine, Cupid Clinic, Iwamizawa, Japan
- KMID: 2540984
- DOI: http://doi.org/10.5115/acb.22.133
Abstract
- It is unclear whether forearm and crural muscle fibers extend distally across the wrist and ankle joints, respectively. We hypothesized, in late-term fetuses, an over-production of muscle bellies extending over the joint. Muscle fibers in histological sections from unilateral wrists and ankles of 16 late-term fetuses (30–40 weeks) were examined and compared with 15 adult cadavers. Muscle fibers of the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) in fetuses, especially muscle bellies to the third and fourth fingers, were found to extend far distally beyond the radiocarpal joint. The extensor digitorum and extensor pollicis longus on the extensor side of the wrist were found to carry distally-extending muscle fibers, but these fibers did not extend beyond the distal end of the radius. In the ankle, most muscle bundles in the flexor hallucis longus (FHL), fibularis brevis (FB) and extensor digitorum longus extended distally beyond the talocrural joint, with most FB muscle fibers reaching the level of the talocalcaneal joint. In adult cadavers, muscle fibers of the FDP and FHL did not reach the levels of the radiocarpal and talocrural joints, respectively, whereas the FB muscle belly always reached the talocalcaneal joint. Similarly, some of the FDS reached the level of the radiocarpal joint. Generally, infants’ movements at the wrist and ankle could result in friction injury to over-extended muscle. However, the calcaneal and FDP tendons might protect the FB and FDS tendons, respectively, from friction stress.
Keyword
Figure
-

Fig. 1 Longitudinal sections of the hand and wrist showing distally extending muscle bellies of the flexor digitorum superficialis in a fetus at 28 weeks. H&E staining. Frontal sections tangential to the hand palmar surface. (A) (most superficial or palmar), (C, D) (deepest or most dorsal) display the proximodistal levels of the MP and CM joints at the lower magnification. (B) A higher magnification view of a square in (A), exhibits distal extensions of the FDS muscle. (A, C, D) were prepared at the same magnification. Between (A, C), the deep flexors also had distal extending muscle bellies (not shown). (A, C, D) were prepared at the same magnification. MP, metacarpopharangeal; CM, carpometacarpal; FDS, flexor digitorum superficialis, FDP, flexor digitorum profundus tendon; LU, lunate; PQ, pronator quadratus muscle; RA, radius; SC, scaphoid; TR, trapezium.

Fig. 2 Transverse sections of the wrist showing distally extending muscle fibers of the long flexors and extensors in a fetus at 32 weeks. H&E staining. A single cross section. (A) displays topographical anatomy of the tendons at the wrist. (B, C) (same magnification) are higher magnification views of squares in (A), respectively. (D, E) (or F, G) are higher magnification views of squares in (B) (or C): these four panels were prepared at the same magnification. Muscle-tendon borders are encircled or indicated by dotted line (B–G). In the carpal tunnel, the 3th and 5th fingers’ bellies of the FDS muscle as well as all four bellies of the FDP muscle extend distally. The lumbricalis muscle appeared in the distal side of the figure. In the extensor side, a deep tendon of the ED muscle as well as the ulnar margin of the EPL muscle carries distally-extending muscle fibers. (B, C) (or D–G) were prepared at the same magnification. BPL, abductor pollicis longus muscle; ECRB, extensor carpi radialis brevis muscle; ECRL, extensor carpi radialis longus muscle; ECU, extensor carpi ulnaris muscle; MN, median nerve; UN, ulnar nerve; MP, metacarpopharangeal; CM, carpometacarpal; FDS, flexor digitorum superficialis; FDP, flexor digitorum profundus; ED, extensor digitorum; EPL, extensor pollicis longus.

Fig. 3 Longitudinal sections of the ankle showing distal extensions of long crural muscle bellies in a late-stage fetus at 30 weeks. H&E staining. Sagittal sections from a fetus at 30 weeks. (A) (or D) displays a medial (or lateral) plane through the ankle.at the ultralow magnification. (B) (or E) is a higher magnification view of a square in panel A (or D). (C) corresponds to a square in (B). In (A–C), a muscle belly of the FHL muscle changes into the tendon at a level below the talocrural joint surfaces. In (D, E), a muscle belly of the FB muscle also extends to a level below the joint surface. Both muscle bellies are adjacent to the joint capsule. (A, D) were prepared at the same magnification. AT, Achillis (or calcaneal) tendon; EHL, extensor hallucis longus tendon; FDL, flexor digitorum longus tendon; PTFL, posterior talofibular ligament; T nerve, tibial nerve; FHL, flexor hallucis longus; FB, fibularis brevis.

Fig. 4 Transverse sections of the ankle showing crural muscle fibers extending distally in a fetus at 31 weeks. H&E staining. Horizontal section. (A) displays a level of the talocrural joint, while (D) exhibits the talocalcaneal joint. (B, C, E) are higher magnification views of squares in (A), respectively, while (F) is that in (D). In the four panels, a muscle tendon border (dotted line) is shown in the FB, EDL, and FHL. (A, D) (or B, C, E, F) were prepared at the same magnification. AT, Achillis (or calcaneal) tendon; FDL, flexor digitorum longus tendon; FL, fibularis longus; PTFL, posterior talofibular ligament; TN, tibial nerve; TP, tibialis posterior; FB, fibularis brevis; EDL, extensor digitorum longus; FHL, flexor hallucis longus.
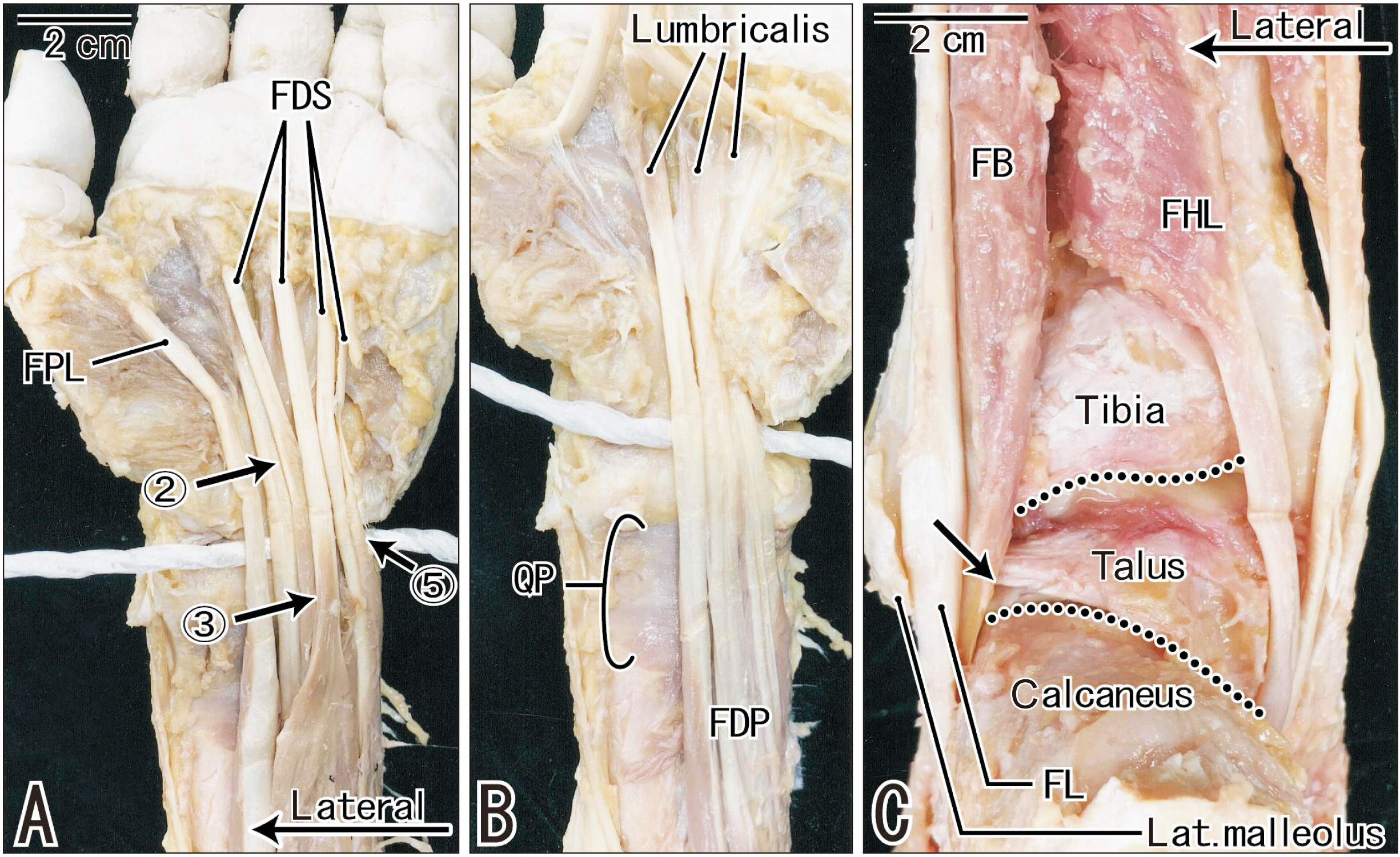
Fig. 5 Macroscopic observations of tendons and muscle bellies at the wrist and ankle of an 86 years-old man. (A) displays the FDS and FPL at the hand and wrist, while (B) exhibits the FDP and QP after removal of the superficial layer. A thick white string indicates a level of the radiocarpal joint surface. Arrows with number indicate the FDS muscle fibers extending across the joint along the tendons to the second, third and fifth fingers. The FDP muscle fibers do not reach a level of the joint (B). (C) is a posterior view of the ankle after removal of Achillis tendon and triceps surae muscles. Two dotted lines indicate the talocrural and talocalcaneal joints, respectively. Behind the lateral malleolus of the fibula, a muscle belly of the FB extends distally along the FL tendon and appears to reach a level of the talocalcaneal joint (arrow). The FHL muscle fibers does not reach the joint. (A, B) were prepared at the same magnification. FDS, flexor digitorum superficialis; FPL, flexor pollicus longus; FDP, flexor digitorum profundus; QP, quadratus plantae; FB, fibularis brevis; FL, fibularis longus; FHL, flexor hallucis longus.
Reference
-
References
1. Spinner M. 1978. Injuries to the major branches of peripheral nerves of the forearm. 2nd ed. Saunders;Philadelphia:2. Neumeister MW, Mowlavi A, Russell RC, Wilhelmi BJ. 2005; Anomalous flexor digitorum superficialis muscle transposition for vascular coverage of the median nerve in recurrent carpal tunnel syndrome. Can J Plast Surg. 13:27–30. DOI: 10.1177/229255030501300102. PMID: 24222998. PMCID: PMC3822475.
Article3. Tubbs RS, Yablick MW, Loukas M, Shoja MM, Ardalan M, Oakes WJ. 2008; Capsular attachment of the brachialis muscle (Portal's muscle): an anatomical and functional study. Surg Radiol Anat. 30:229–32. DOI: 10.1007/s00276-008-0312-y. PMID: 18253690.
Article4. Sanal HT, Chen L, Negrao P, Haghighi P, Trudell DJ, Resnick DL. 2009; Distal attachment of the brachialis muscle: anatomic and MRI study in cadavers. AJR Am J Roentgenol. 192:468–72. DOI: 10.2214/AJR.08.1150. PMID: 19155412.
Article5. Jin ZW, Jin Y, Yamamoto M, Abe H, Murakami G, Yan TF. 2016; Oblique cord (chorda obliqua) of the forearm and muscle-associated fibrous tissues at and around the elbow joint: a study of human foetal specimens. Folia Morphol (Warsz). 75:493–502. DOI: 10.5603/FM.a2016.0019. PMID: 27830875.
Article6. Abe S, Aoki M, Nakao T, Kasahara M, Rodriguez-Vazquez JF, Murakami G, Cho BH. 2014; Variation of the subscapularis tendon at the fetal glenohumeral joint. Okajimas Folia Anat Jpn. 90:89–95. DOI: 10.2535/ofaj.90.89. PMID: 24815107.
Article7. Muraki T, Aoki M, Uchiyama E, Takasaki H, Murakami G, Miyamoto S. 2007; A cadaveric study of strain on the subscapularis muscle. Arch Phys Med Rehabil. 88:941–6. DOI: 10.1016/j.apmr.2007.04.003. PMID: 17601478.
Article8. Jin ZW, Kim JH, Suzuki D, Sugai N, Murakami G, Abe H, Rodríguez-Vázquez JF. 2021; Relationship of the fabella with the origins of the plantaris and gastrocnemius lateral head muscles in late-term fetuses: a histological study. Anat Cell Biol. 54:270–9. DOI: 10.5115/acb.20.326. PMID: 33896799. PMCID: PMC8225468.
Article9. Tidball JG. 1992; Desmin at myotendinous junctions. Exp Cell Res. 199:206–12. DOI: 10.1016/0014-4827(92)90425-8. PMID: 1544366.
Article10. Carlsson L, Li Z, Paulin D, Thornell LE. 1999; Nestin is expressed during development and in myotendinous and neuromuscular junctions in wild type and desmin knock-out mice. Exp Cell Res. 251:213–23. DOI: 10.1006/excr.1999.4569. PMID: 10438587.
Article11. Trotter JA. 1993; Functional morphology of force transmission in skeletal muscle. A brief review. Acta Anat (Basel). 146:205–22. DOI: 10.1159/000147459. PMID: 8317197.12. Huijing PA. 1999; Muscle as a collagen fiber reinforced composite: a review of force transmission in muscle and whole limb. J Biomech. 32:329–45. DOI: 10.1016/S0021-9290(98)00186-9. PMID: 10213024.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influence of developing ligaments on the muscles in contact with them: a study of the annular ligament of the radius and the sacrospinous ligament in mid-term human fetuses
- Insertions of the striated muscles in the skin and mucosa: a histological study of fetuses and cadavers
- Distribution of elastic fibers in the head and neck: a histological study using late-stage human fetuses
- Striated muscle fiber crossings of the head and neck: a histological study using near-term human fetuses and elderly cadavers
- MR Image Findings of Giant Cell Tumor of the Tendon Sheath Involving the Foot: A Case Report
