Parenchyma-preserving hepatectomy including segments I + IV resection and bile duct resection in a patient with type IV perihilar cholangiocarcinoma: A case report with video clip
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2519302
- DOI: http://doi.org/10.14701/ahbps.2021.25.3.419
Abstract
- It has been reported that parenchyma-preserving hepatectomy (PPH) might lower surgical curability with an increased likelihood of bile duct resection margins (BDRMs). Apparently, PPH is indicated for patients expected to achieve curative resection. The author herein presents a case of a 77-year-old male patient with type IV perihilar cholangiocarcinoma and decreased cardiac function treated with hepatic segments I + IV resection and bile duct resection. During the operation, he underwent two hepatic parenchymal transections matched with right trisectionectomy and left hepatectomy. After removing segments VI and I and extrahepatic bile duct, six hepatic duct openings were exposed at the left and right hila. As some of them were conjoined, two hepaticojejunostomies at the right liver and one hepaticojejunostomy at the left lateral section were performed consecutively. This operation took 7 hours. Eight sessions of intraoperative frozen-section biopsy were performed. All BDRMs were tumor-negative. According to the 8th edition of the American Joint Committee on Cancer staging system, the extent of the tumor was pT2bN2M0. It was regarded as stage IVA tumor. The patient recovered uneventfully. He was discharged on the 18th postoperative day. The patient underwent concurrent chemoradiation therapy and adjuvant chemotherapy. The patient has been doing well without tumor recurrence for the past 24 months to date. In conclusion, PPH can lead to curative resection and improved outcomes through reasonable adjustment of the extent of hepatectomy.
Keyword
Figure
-
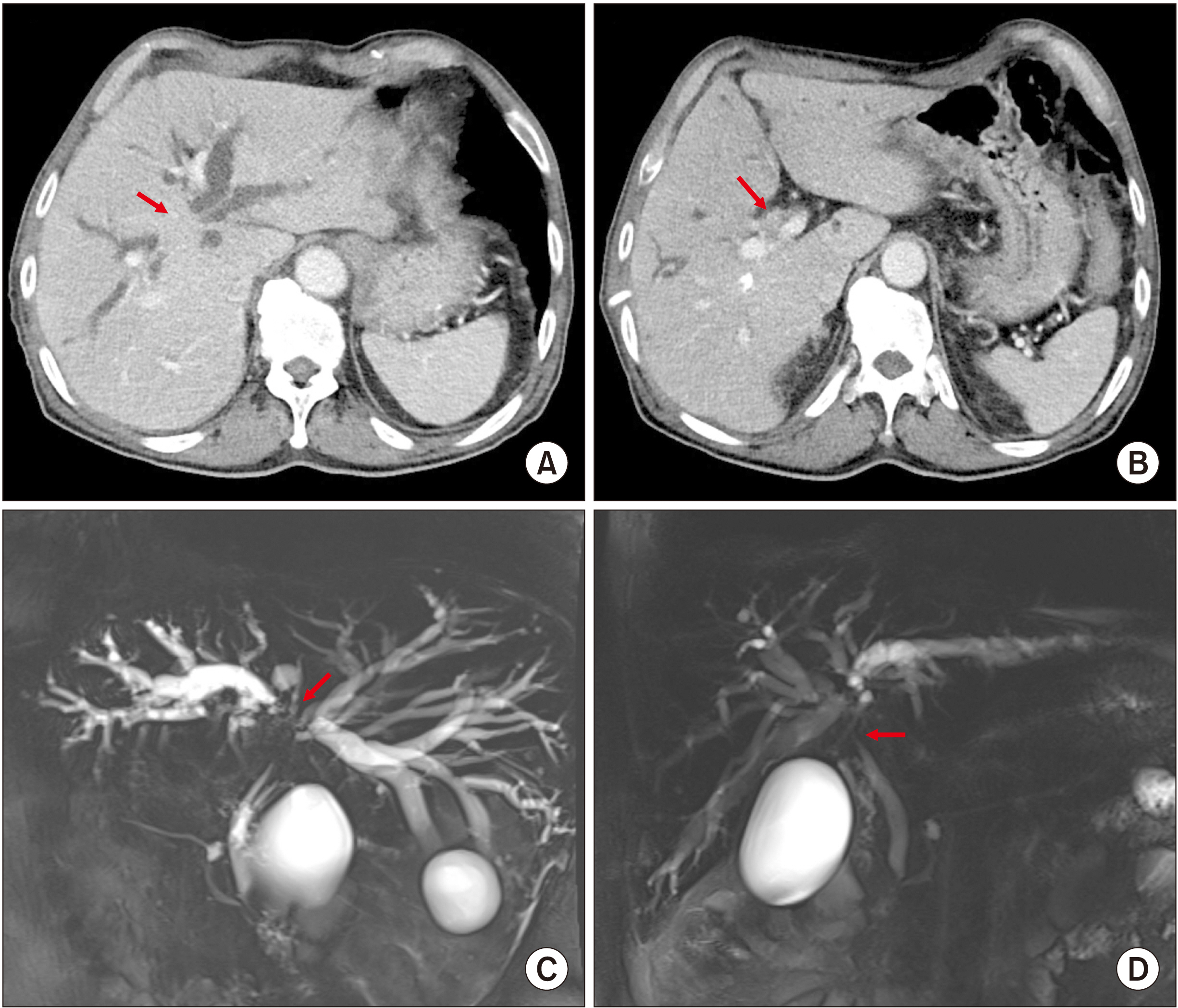
Fig. 1 Preoperative imaging study findings. Computed tomography images (A, B) and magnetic resonance cholangiography images (C, D) show extensive hilar bile duct obstruction, suggesting perihilar cholangiocarcinoma of Bismuth-Corlette type IV. Arrows indicate tumor.
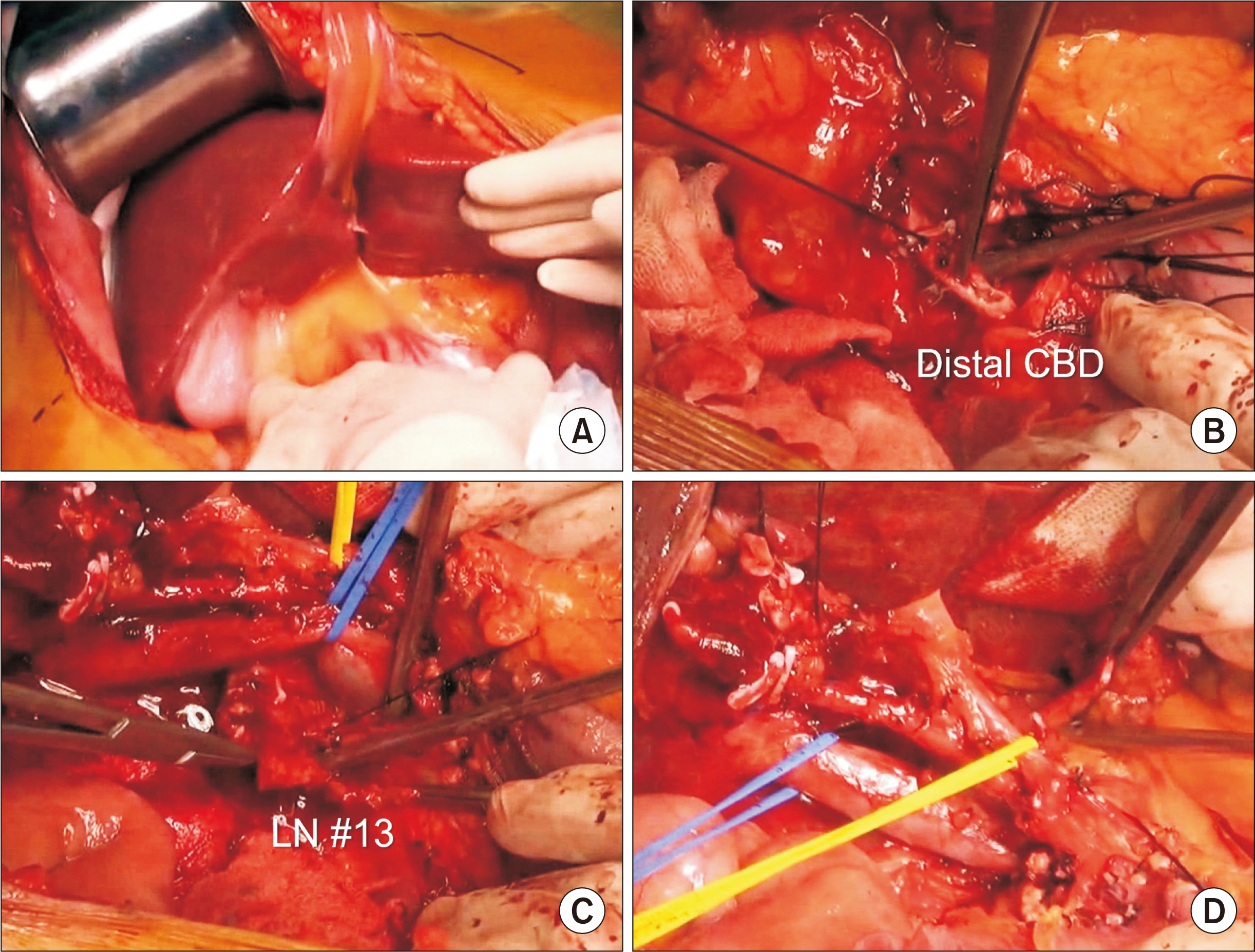
Fig. 2 Intraoperative photographs showing dissection of the hepatoduodenal ligament. Surgical resectability is assessed through manual palpation (A). The distal common bile duct (CBD) is transected (B). Enlarged regional lymph nodes (LNs) are dissected (C). Intraoperative frozen-section biopsy showed nodal metastasis. The hepatic artery and portal vein branches are isolated without macroscopic vascular invasion (D).
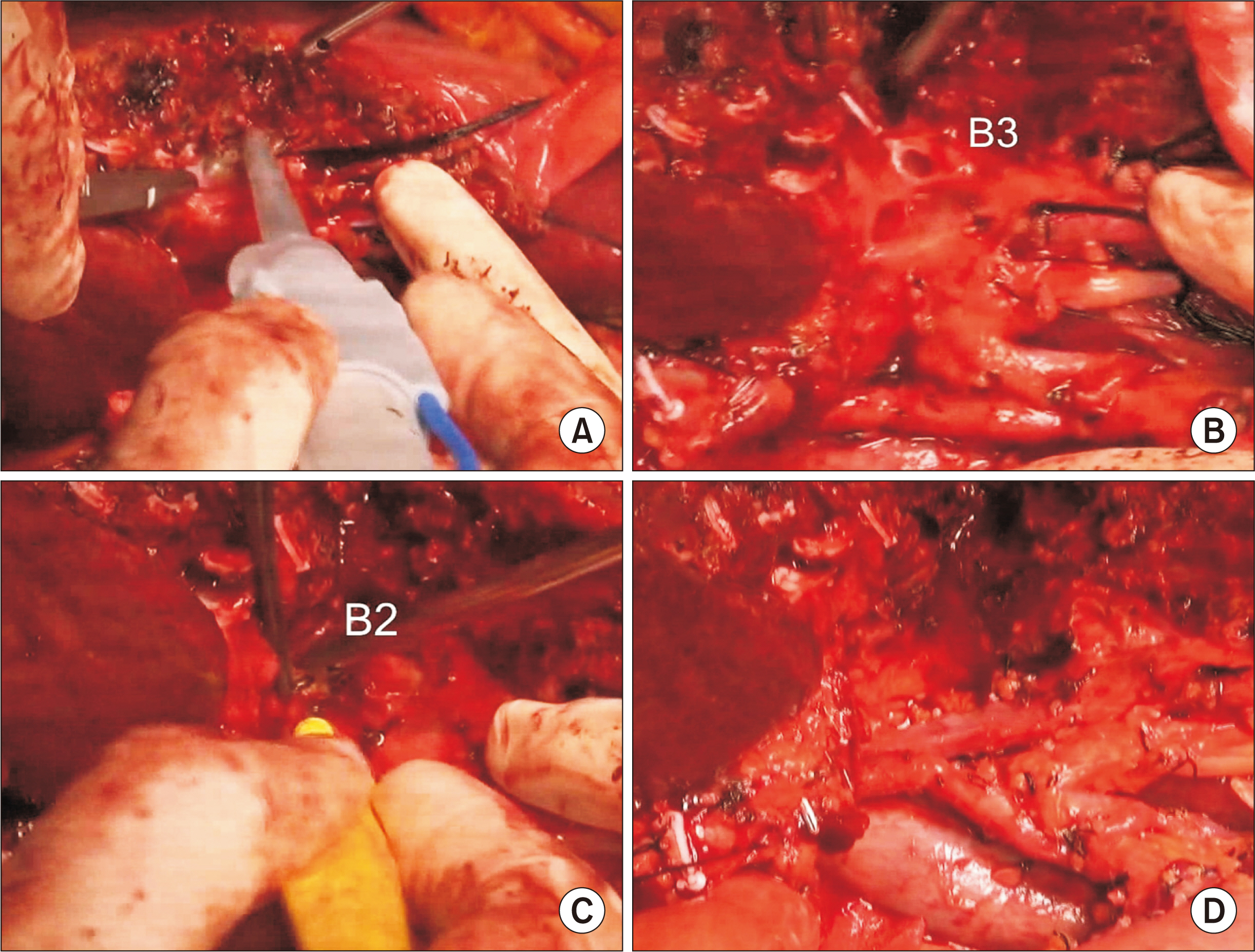
Fig. 3 Intraoperative photographs showing left liver transection. The liver parenchyma is transected along the falciform ligament (A). The segment III duct (B3) and segment II duct (B2) are consecutively transected (B, C). The left portal vein and hepatic artery are further dissected to expose the umbilical portion of the left portal vein, and the remnant left lateral segment is separated from the left caudate lobe (D).
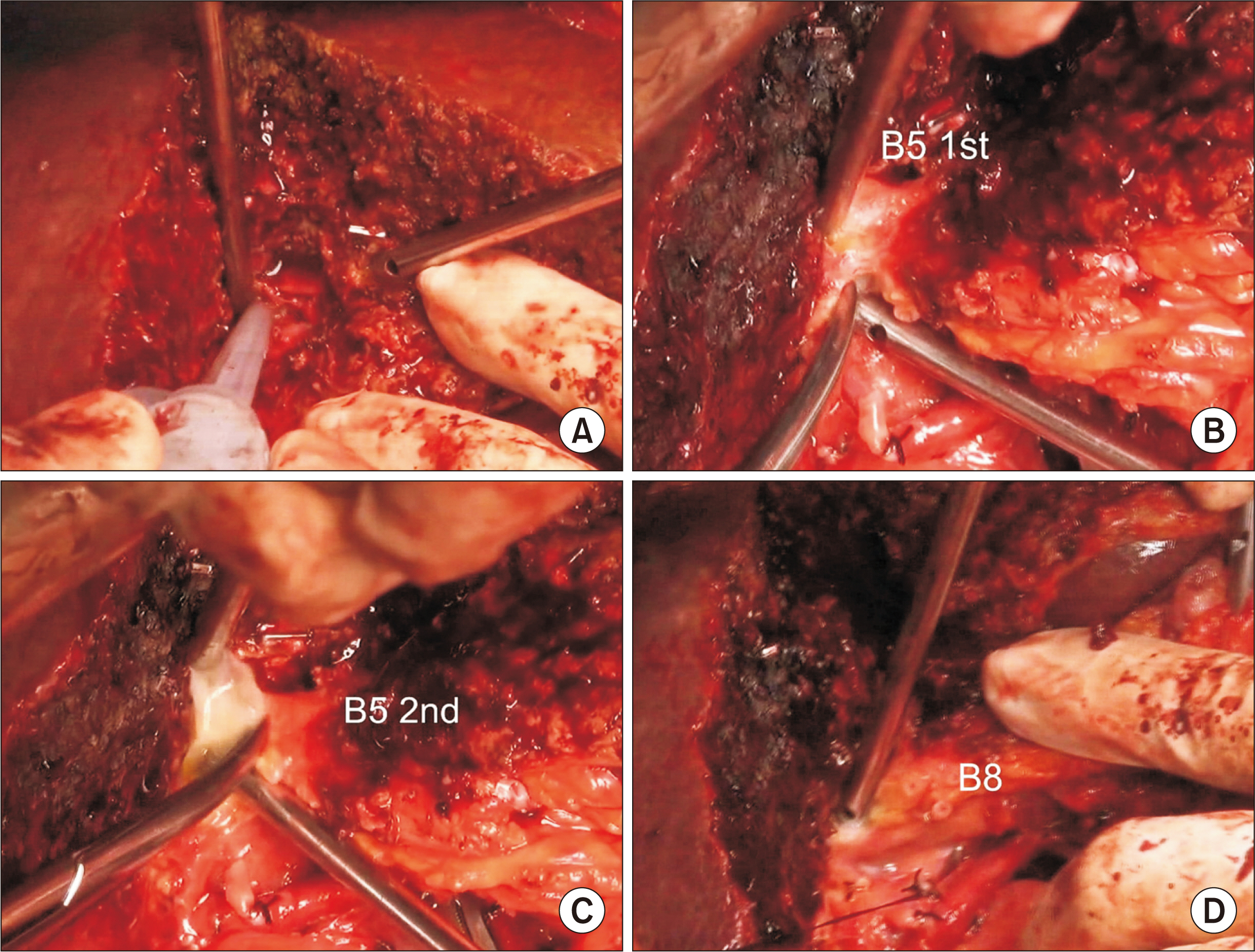
Fig. 4 Intraoperative photographs showing right liver transection. Right-sided hepatic parenchymal transection is performed along the hemi-liver discoloration line (A). Two segment V ducts (B5) are transected (B, C). Segment VIII duct (B8) is transected (D).
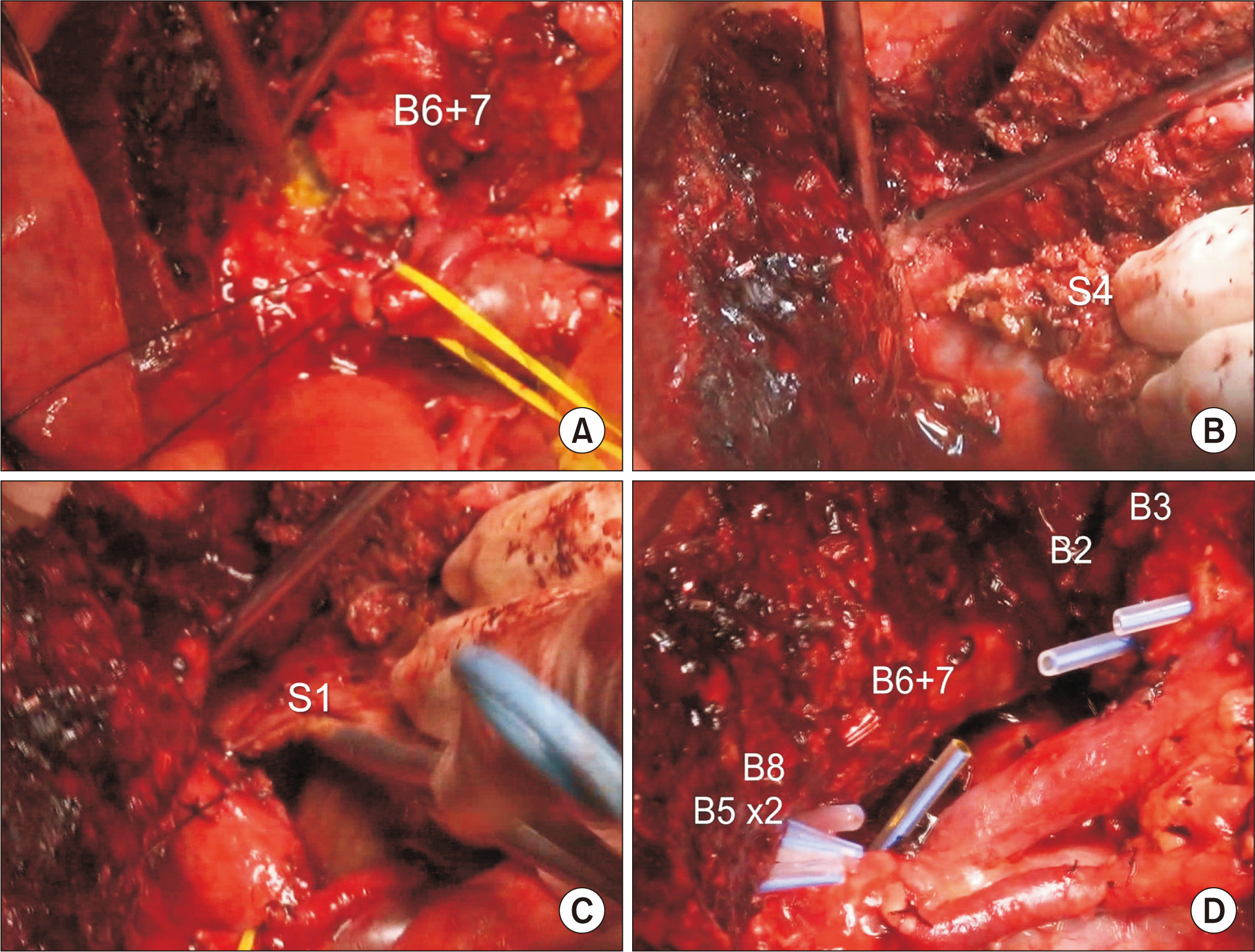
Fig. 5 Intraoperative photographs showing right liver transection. Conjoined segments VI and VII duct (B6 + 7) is transected (A). The paracaval portion and the left caudate lobe (S1) are removed along with segment IV (S4) resection (B, C). There are six hepatic duct openings at the left and right hila (D).
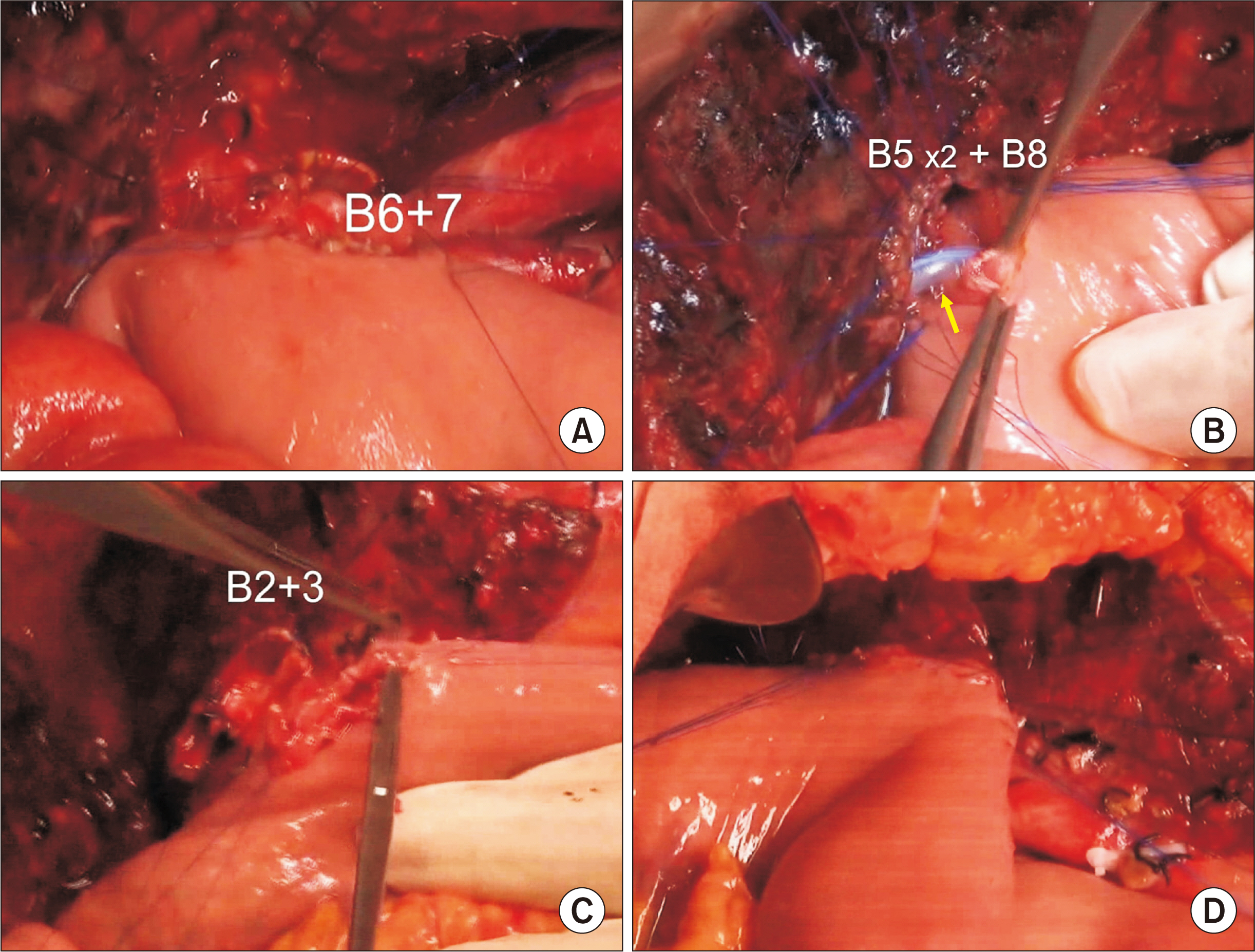
Fig. 6 Intraoperative photographs showing biliary reconstruction. Segments VI and VII duct (B6 + 7) is reconstructed through a single hepaticojejunostomy (HJ) (A). Two segment V ducts (B5) and one segment VIII duct (B8) are conjoined and a single HJ is performed with stent insertion into the small B5 duct (arrow) (B). Segment II and III ducts (B2 + 3) are conjoined and a single HJ is performed (C, D).

Fig. 7 Gross photograph of the resected specimen with segments VI and I and the extrahepatic bile duct.
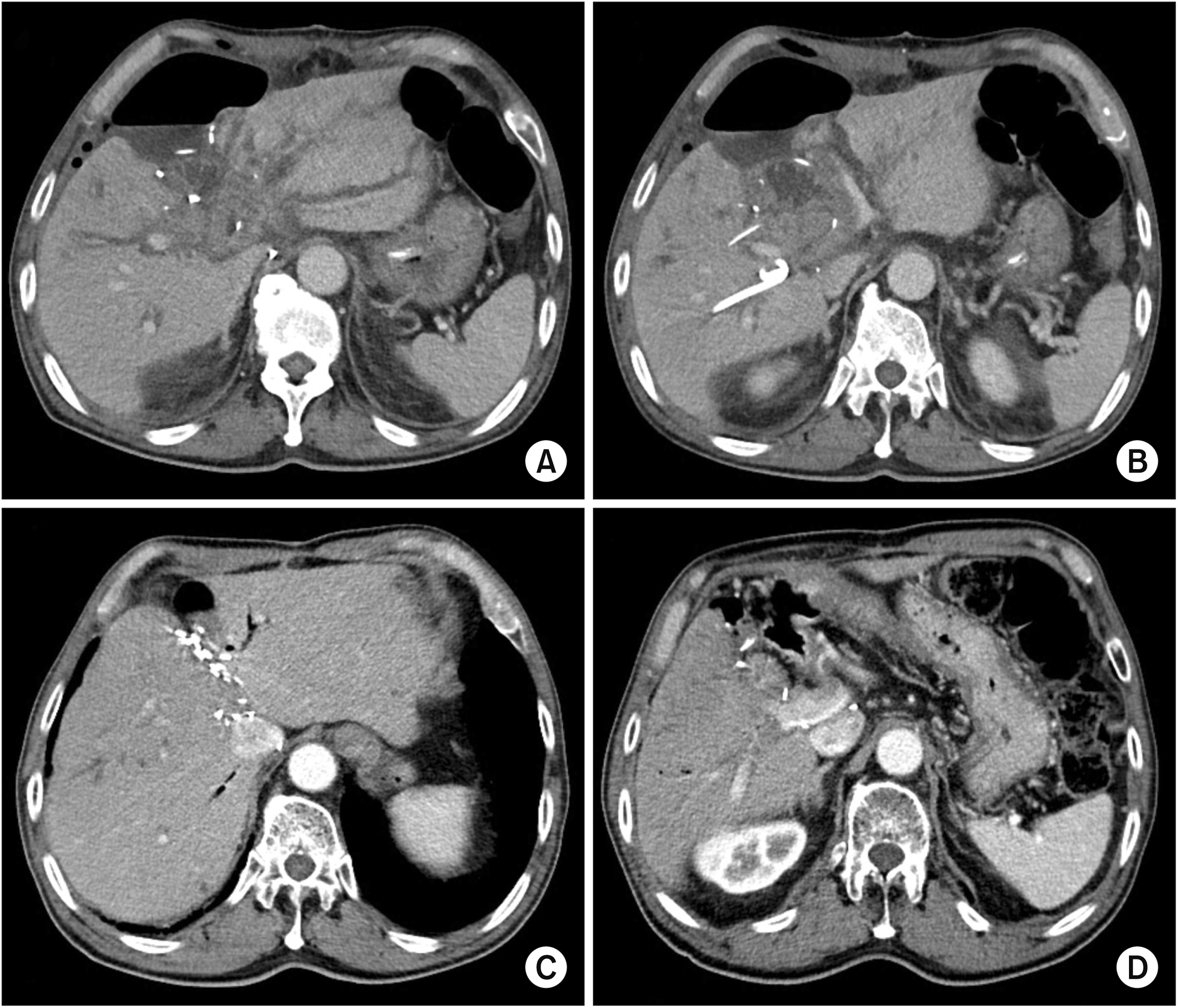
Fig. 8 Postoperative computed tomography findings. Images taken 10 days (A, B) and 18 months (C, D) after surgery show no abnormal findings.
Reference
-
1. Baer HU, Stain SC, Dennison AR, Eggers B, Blumgart LH. 1993; Improvements in survival by aggressive resections of hilar cholangiocarcinoma. Ann Surg. 217:20–27. DOI: 10.1097/00000658-199301000-00005. PMID: 8380975. PMCID: PMC1242729.
Article2. Childs T, Hart M. 1993; Aggressive surgical therapy for Klatskin tumors. Am J Surg. 165:554–557. DOI: 10.1016/S0002-9610(05)80433-7. PMID: 7683844.
Article3. Tsuzuki T, Ueda M, Kuramochi S, Iida S, Takahashi S, Iri H. 1990; Carcinoma of the main hepatic duct junction: indications, operative morbidity and mortality, and long-term survival. Surgery. 108:495–501. PMID: 2396193.4. Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. 1990; Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 14:535–543. discussion 544DOI: 10.1007/BF01658686. PMID: 2166381.
Article5. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Shimizu Y, et al. 1998; Aggressive surgical approaches to hilar cholangiocarcinoma: hepatic or local resection? Surgery. 123:131–136. DOI: 10.1016/S0039-6060(98)70249-1. PMID: 9481397.
Article6. Iida S, Tsuzuki T, Ogata Y, Yoneyama K, Iri H, Watanabe K. 1987; The long-term survival of patients with carcinoma of the main hepatic duct junction. Cancer. 60:1612–1619. DOI: 10.1002/1097-0142(19871001)60:7<1612::AID-CNCR2820600732>3.0.CO;2-1. PMID: 3621131.
Article7. Hayashi S, Miyazaki M, Kondo Y, Nakajima N. 1994; Invasive growth patterns of hepatic hilar ductal carcinoma. A histologic analysis of 18 surgical cases. Cancer. 73:2922–2929. DOI: 10.1002/1097-0142(19940615)73:12<2922::AID-CNCR2820731208>3.0.CO;2-K. PMID: 8199989.
Article8. Blumgart LH, Hadjis NS, Benjamin IS, Beazley R. 1984; Surgical approaches to cholangiocarcinoma at confluence of hepatic ducts. Lancet. 1:66–70. DOI: 10.1016/S0140-6736(84)90002-3. PMID: 6197596.
Article9. Miyazaki M, Itoh H, Ambiru S, Shimizu H, Togawa A, Gohchi E, et al. 1996; Radical surgery for advanced gallbladder carcinoma. Br J Surg. 83:478–481. DOI: 10.1002/bjs.1800830413. PMID: 8665234.
Article10. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Okaya T, et al. 1999; Parenchyma-preserving hepatectomy in the surgical treatment of hilar cholangiocarcinoma. J Am Coll Surg. 189:575–583. DOI: 10.1016/S1072-7515(99)00219-7. PMID: 10589594.
Article11. Lee SG, Hwang S. 2005; How I do it: assessment of hepatic functional reserve for indication of hepatic resection. J Hepatobiliary Pancreat Surg. 12:38–43. DOI: 10.1007/s00534-004-0949-9. PMID: 15754098.
Article12. Hwang S, Ha TY, Ko GY, Kwon DI, Song GW, Jung DH, et al. 2015; Preoperative sequential portal and hepatic vein embolization in patients with hepatobiliary malignancy. World J Surg. 39:2990–2998. DOI: 10.1007/s00268-015-3194-2. PMID: 26304608.
Article13. Klempnauer J, Ridder GJ, Werner M, Weimann A, Pichlmayr R. 1997; What constitutes long-term survival after surgery for hilar cholangiocarcinoma? Cancer. 79:26–34. DOI: 10.1002/(SICI)1097-0142(19970101)79:1<26::AID-CNCR5>3.0.CO;2-K. PMID: 8988723.14. Klempnauer J, Ridder GJ, von Wasielewski R, Werner M, Weimann A, Pichlmayr R. 1997; Resectional surgery of hilar cholangiocarcinoma: a multivariate analysis of prognostic factors. J Clin Oncol. 15:947–954. DOI: 10.1200/JCO.1997.15.3.947. PMID: 9060532.
Article15. Mizumoto R, Kawarada Y, Suzuki H. 1986; Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obstet. 162:153–158. PMID: 3945893.16. Hwang S, Ha TY, Kim JS, Kim KH, Lee SG, Lee YJ, et al. 2003; Isolated caudate lobectomy with bile duct resection performed in a patient with type IV hilar bile duct cancer. J Korean Surg Soc. 64:441–446.17. Hwang S, Moon DB, Park EH, Kim MH, Lee YJ, Lee SG. 2003; S4a+S5 with caudate lobe (S1) resection as a parenchyma-preserving liver resection for a patient with type IIIb hilar bile duct cance. J Korean Surg Soc. 64:515–520.18. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Shimizu Y, et al. 1998; Segments I and IV resection as a new approach for hepatic hilar cholangiocarcinoma. Am J Surg. 175:229–231. DOI: 10.1016/S0002-9610(97)00295-X. PMID: 9560126.
Article19. Lee SG, Song GW, Hwang S, Ha TY, Moon DB, Jung DH, et al. 2010; Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci. 17:476–489. DOI: 10.1007/s00534-009-0204-5. PMID: 19851704.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Standard and modified techniques for parenchyma-preserving hepatectomy focused on segments I+IV resection in patients with perihilar cholangiocarcinoma
- Necrosectomy of hepatic left lateral section after blunt abdominal trauma in a patient who underwent central hepatectomy and bile duct resection for perihilar cholangiocarcinoma
- Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
- S4a+S5 with Caudate Lobe (S1) Resection as a Parenchyma-preserving Liver Resection for a Patient with Type IIIb Hilar Bile Duct Cance
- Spontaneous rupture of intrahepatic bile duct following portal vein embolization in a patient with perihilar cholangiocarcinoma: a case of successful curative resection
