Standard and modified techniques for parenchyma-preserving hepatectomy focused on segments I+IV resection in patients with perihilar cholangiocarcinoma
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2513184
- DOI: http://doi.org/10.14701/ahbps.2021.25.1.112
Abstract
- Resection of the hepatic segments I+IV (S1+S4) is the most common type of parenchyma-preserving hepatectomy (PPH) for perihilar cholangiocarcinoma (PHCC). The author describes personal experience on the standard and modified techniques for PPH focused on S1+S4 resection in patients with PHCC. 1) Isolated caudate lobectomy with bile duct resection (BDR) is the minimal type of PPH, but not currently recommended due to technical difficulty. 2) Partial hepatectomy of S1+S4a±segment V (S5) with BDR provides wide operative field, but extension of BDR is limited and resection of S1 paracaval portion is still difficult. 3) Resection of S1+S4+S5 with BDR provides wider operative field for complete S1 resection and multiple biliary reconstruction. 4) Resection of S1+S4 with BDR offers very wide operative field and allows wider extent of hilar BDR, and thus presents the most common type of PPH. A supplementary video clip presents the detailed standard surgical procedure for resection of S1+S4 with BDR in a patient with type IIIA PHCC. 5) Modified resection of S1+S4±S5 or segment VIII (S8) with BDR facilitates additional resection of tumor-involved S5 or S8 ducts. 6) Major hilar vascular invasion is usually contraindicated for PPH and only small portal vein invasion requiring wedge resection and patch venoplasty is allowed. In conclusion, PPH can achieve curative resection and improved outcomes in patients with PHCC via reasonable modification of the extent of hepatectomy and hilar BDR. PPH may have advantages in selected patients depending on the extent of tumor, and in patients with high operative risk
Keyword
Figure
-
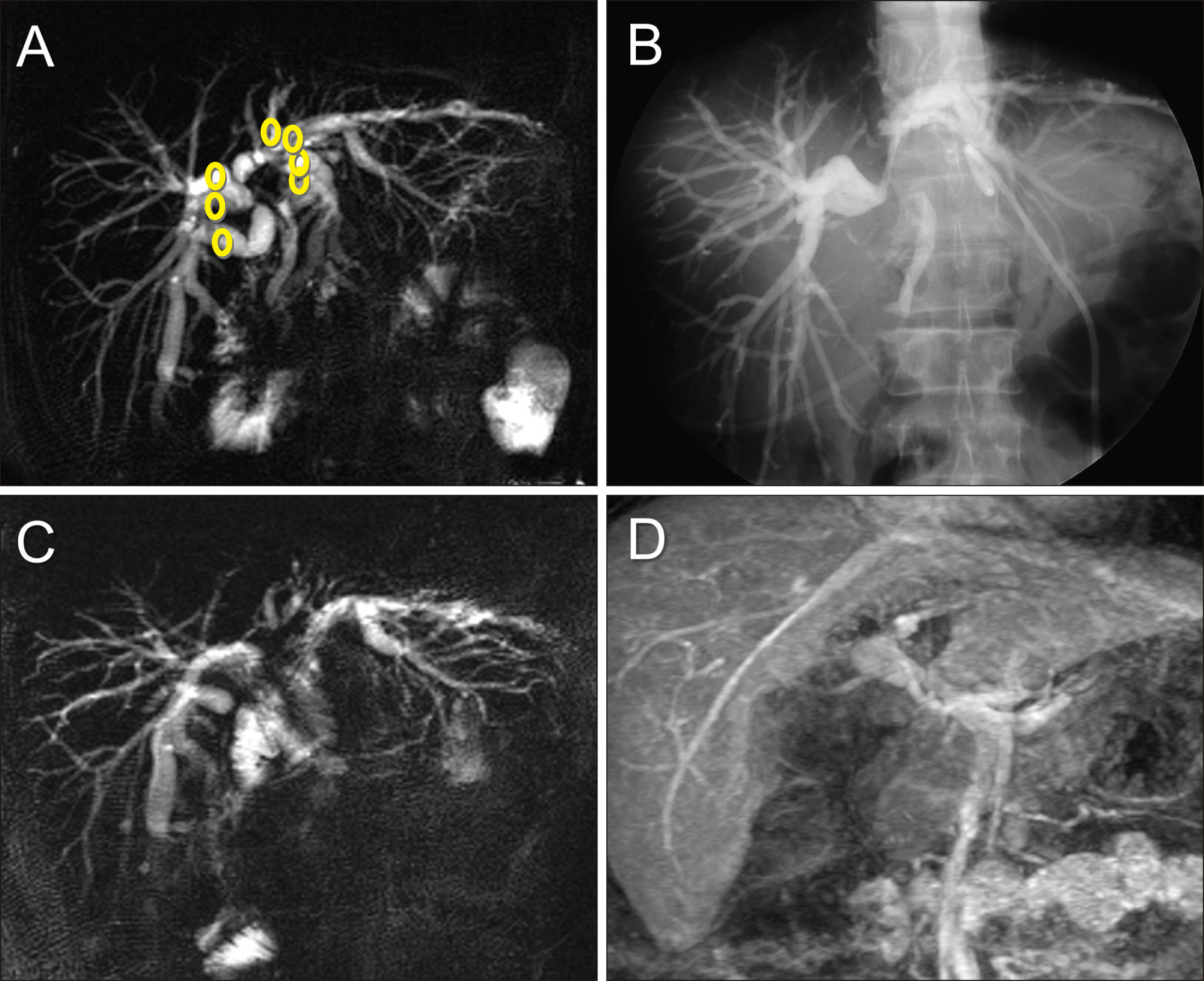
Fig. 1 Perioperative findings of isolated caudate lobectomy and bile duct resection. (A, B) Preoperative magnetic resonance and direct tube cholangiography images show type IV perihilar cholangiocarcinoma. Circles indicate the individual locations of bile duct transection. (C, D) Postoperative magnetic resonance images taken 4 weeks after surgery show the uneventful status of multiple hepaticojeunostomies and the extent of hepatic parenchymal resection.

Fig. 2 Intraoperative Intraoperative photographs showing resection of the segments I+IV+V. (A, B) The segments IV and V are partially resected, and then the paracaval portion and Spigelian lobe of the caudate lobe are resected partially in a patient with type II perihilar cholangiocarcinoma. Multiple bile duct openings are exposed after hilar bile duct resection. (C, D) In another patient with type I perihilar cholangiocarcinoma, the segments IV and V are partially resected concurrently with the Spigelian lobe. The shape of the resected specimen indicates the extent of surgical resection.

Fig. 3 Intraoperative photographs showing the extent of hepatectomy following resection of the segments I+IVa+V in a patient with type IIIB perihilar cholangiocarcinoma. (A) The hepatoduodenal ligament was skeletonized. (B) Resection of the segments I+IVa+V is performed with preservation of the middle hepatic vein trunk. Silastic stents are inserted in the multiple bile duct openings. (C) The resected specimen is visible, indicating the extent of surgical resection. (D) Single hepaticojejunstomy involves each of the right- and left-sided conjoined ducts.
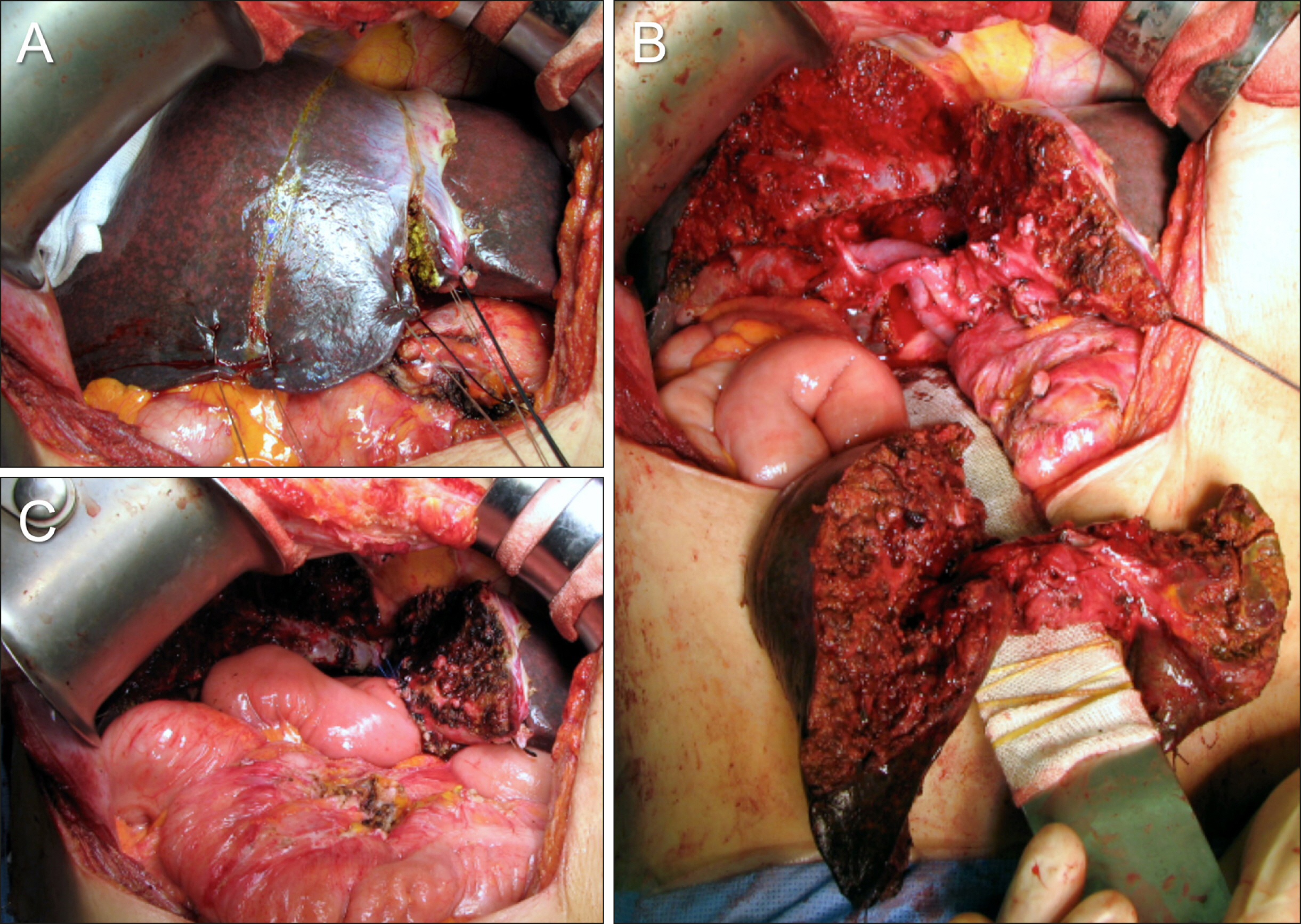
Fig. 4 Intraoperative photographs showing the extent of hepatectomy following resection of the segments I+IV in a patient with type II perihilar cholangiocarcinoma. (A) The extent of segment IV resection is marked at the liver surface. (B) The surgical specimen shows resection of the segments I+IV and bile duct resection. The middle hepatic vein trunk is completely preserved with excavation of the paracaval portion of the caudate lobe. (C) Two hepaticojejunstomies involving the right-sided conjoined ducts and one involving the left- sided conjoined ducts are shown.

Fig. 5 Intraoperative photographs showing anatomical variations observed during resection of the segments I+IV. (A) Type III portal vein anomaly is visible. (B) Early branching of the segment V duct (B5) is visible (arrow). This anatomy of the right hepatic duct required three separate hepaticojejunostomies, each to the B5, segment VIII duct (B8) and segments VI+VII duct (B6+7). (C) The ventral end of the middle hepatic vein trunk is not dissected to protect the fissural vein at the remnant segment IV parenchyma. (D) The middle hepatic vein trunk is transected to remove the paracaval portion of the caudate lobe completely.

Fig. 6 Intraoperative photographs showing additional resection to the usual segments I+IV resection. (A) One branch of the segment V ducts is resected with the corresponding hepatic parenchyma. An arrow indicates the resected branch stump. (B) One branch of the segment VIII ducts is resected with the corresponding hepatic parenchyma (arrow). (C) The medial part of the right anterior section is resected with exposure of the right hepatic vein (arrow). (D) Most of the right anterior section is resected along with exposure of the right hepatic vein (arrow).

Fig. 7 Intraoperative photographs showing vascular reconstruction combined with resection of the segments I+IV. (A, B) The left portal vein is invaded by the tumor, warranting wedge resection and venoplasty using an iliac vein allograft patch. (C) An iliac vein allograft (arrow) is interposed at the left portal vein. (D) The right hepatic artery is interposed with an autologous greater saphenous vein graft conduit (bidirectional arrow).
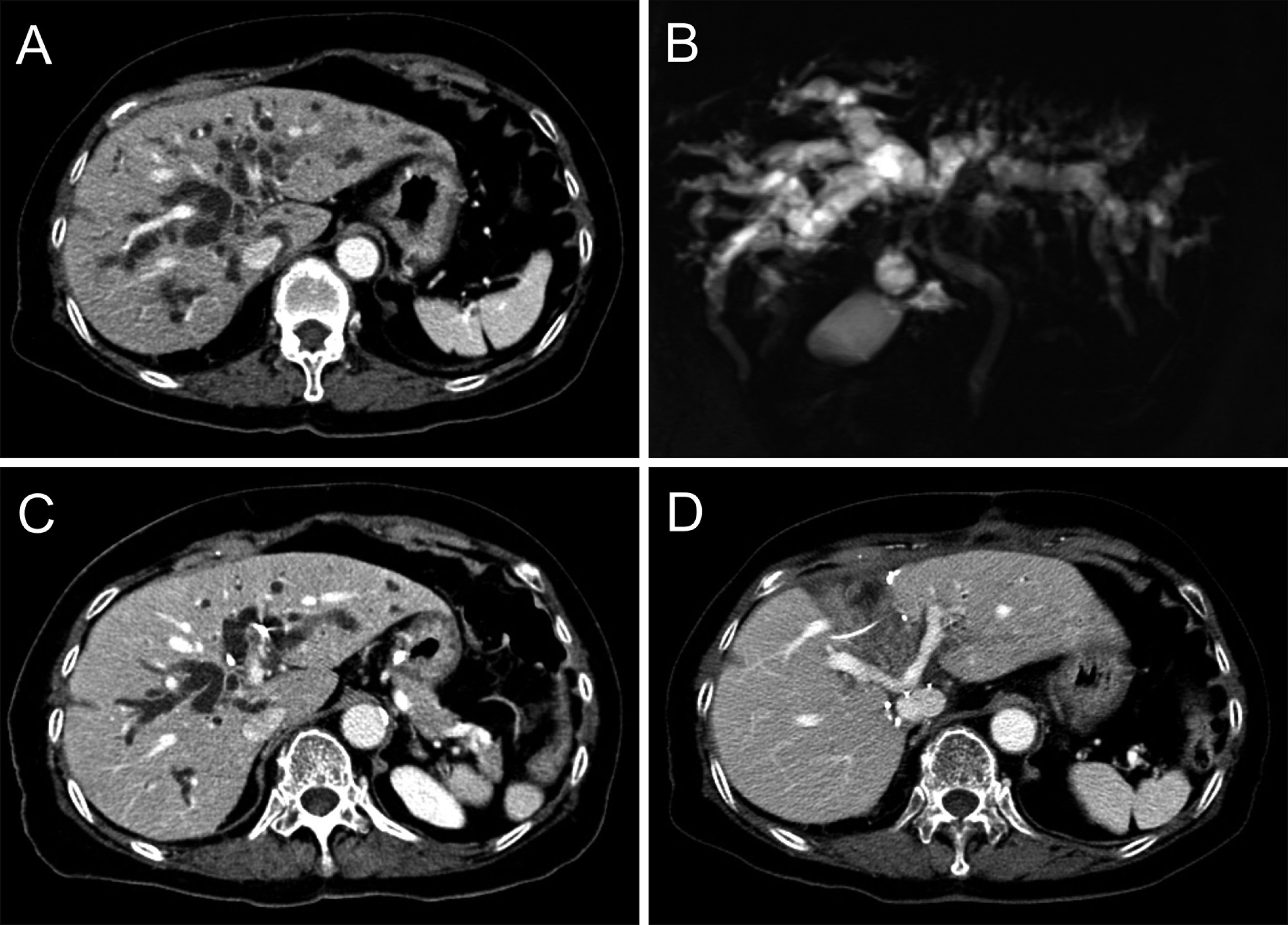
Fig. 8 Perioperative findings of segments I+IV resection and bile duct resection in a 75-year-old male patient with type IIIA perihilar cholangiocarcinoma. (A, B) Preoperative computed tomography and magnetic resonance cholangiography taken before biliary decompression show marked dilatation of all intrahepatic ducts. (C) Preoperative computed tomography taken after biliary decompression still reveals marked dilatation of the intrahepatic ducts. (D) Computed tomography taken 2 weeks after resection of segments I+IV shows no abnormal findings.

Fig. 9 Intraoperative photographs showing the surgical procedure for resection of segments I+IV and bile duct. (A) The hepatic artery is encircled after transection of the distal bile duct. (B) The liver surface is marked to define the territory of hepatic resection. (C) The liver parenchyma was transected along the falciform ligament and the left lateral section ducts are transected (arrow). (D) The remnant left lateral section is completely separated from the left caudate lobe.

Fig. 10 Intraoperative photographs showing the surgical procedure for resection of segments I+IV and bile duct. (A) The right-sided hepatic parenchymal transection is performed along the hemi-liver discoloration line. (B) The right anterior and posterior section ducts are transected (arrow). (C) The segment IV parenchyma is separated from the right and left remnant livers. (D) The resected specimen includes the segments I+IV, gallbladder and extrahepatic bile duct.

Fig. 11 Intraoperative photographs showing the surgical procedure for segments I+IV resection and bile duct resection. (A) The opening of the right anterior section duct is conjoined with the opening of the right posterior duct via unification ductoplasty (arrow). (B) Openings of the 4 right hepatic ducts and 3 left hepatic ducts are exposed. Silastic tubes are inserted to identify the duct openings. (C) The 4-cm- wide conjoined right hepatic duct opening is reconstructed by single hepaticojejunostomy. (D) The 2.5-cm-wide left hepatic duct opening is reconstructed by single hepaticojejunostomy.
Cited by 1 articles
-
Intraductal tubulopapillary neoplasms of the pancreas and biliary tract: The black swan of hepatobiliary surgery
Jilyan Decker, Amanda Cavanaugh, Megan Brown, Saverio Ligato, Oscar Kenneth Serrano
Ann Hepatobiliary Pancreat Surg. 2021;25(4):556-561. doi: 10.14701/ahbps.2021.25.4.556.
Reference
-
1. Baer HU, Stain SC, Dennison AR, Eggers B, Blumgart LH. 1993; Improvements in survival by aggressive resections of hilar cholangiocarcinoma. Ann Surg. 217:20–27. DOI: 10.1097/00000658-199301000-00005. PMID: 8380975. PMCID: PMC1242729.
Article2. Childs T, Hart M. 1993; Aggressive surgical therapy for Klatskin tumors. Am J Surg. 165:554–557. DOI: 10.1016/S0002-9610(05)80433-7. PMID: 7683844.
Article3. Tsuzuki T, Ueda M, Kuramochi S, Iida S, Takahashi S, Iri H. 1990; Carcinoma of the main hepatic duct junction: indications, operative morbidity and mortality, and long-term survival. Surgery. 108:495–501. PMID: 2396193.4. Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S. 1990; Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg. 14:535–543. discussion 544DOI: 10.1007/BF01658686. PMID: 2166381.
Article5. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Shimizu Y, et al. 1998; Aggressive surgical approaches to hilar cholangiocarcinoma: hepatic or local resection? Surgery. 123:131–136. DOI: 10.1016/S0039-6060(98)70249-1. PMID: 9481397.
Article6. Iida S, Tsuzuki T, Ogata Y, Yoneyama K, Iri H, Watanabe K. 1987; The long-term survival of patients with carcinoma of the main hepatic duct junction. Cancer. 60:1612–1619. DOI: 10.1002/1097-0142(19871001)60:7<1612::AID-CNCR2820600732>3.0.CO;2-1. PMID: 3621131.
Article7. Hayashi S, Miyazaki M, Kondo Y, Nakajima N. 1994; Invasive growth patterns of hepatic hilar ductal carcinoma. A histologic analysis of 18 surgical cases. Cancer. 73:2922–2929. DOI: 10.1002/1097-0142(19940615)73:12<2922::AID-CNCR2820731208>3.0.CO;2-K. PMID: 8199989.
Article8. Blumgart LH, Hadjis NS, Benjamin IS, Beazley R. 1984; Surgical approaches to cholangiocarcinoma at confluence of hepatic ducts. Lancet. 1:66–70. DOI: 10.1016/S0140-6736(84)90002-3. PMID: 6197596.
Article9. Miyazaki M, Itoh H, Ambiru S, Shimizu H, Togawa A, Gohchi E, et al. 1996; Radical surgery for advanced gallbladder carcinoma. Br J Surg. 83:478–481. DOI: 10.1002/bjs.1800830413. PMID: 8665234.
Article10. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Okaya T, et al. 1999; Parenchyma-preserving hepatectomy in the surgical treatment of hilar cholangiocarcinoma. J Am Coll Surg. 189:575–583. DOI: 10.1016/S1072-7515(99)00219-7. PMID: 10589594.
Article11. Hwang S. Parenchyma-preserving hepatectomy including segment IV+I resection in a patient with type IV perihilar cholangiocarcinoma: A case report with video clip. [in press].
Article12. Hwang S, Ha TY, Kim JS, Kim KH, Lee SG, Lee YJ. 2003; Isolated caudate lobectomy with bile duct resection performed in a patient with type IV hilar bile duct cancer. J Korean Surg Soc. 64:441–446.13. Kawarada Y, Isaji S, Taoka H, Tabata M, Das BC, Yokoi H. 1999; S4a+S5 with caudate lobe (S1) resection using the Taj Mahal liver parenchymal resection for carcinoma of the biliary tract. J Gastrointest Surg. 3:369–373. DOI: 10.1016/S1091-255X(99)80052-3. PMID: 10482688.14. Hwang S, Moon DB, Park EH, Kim MH, Lee YJ, Lee SG. 2003; S4a+S5 with caudate lobe (S1) resection as a parenchyma-preserving liver resection for a patient with type IIIb hilar bile duct cancer. J Korean Surg Soc. 64:515–520.15. Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Shimizu Y, et al. 1998; Segments I and IV resection as a new approach for hepatic hilar cholangiocarcinoma. Am J Surg. 175:229–231. DOI: 10.1016/S0002-9610(97)00295-X. PMID: 9560126.
Article16. Klempnauer J, Ridder GJ, Werner M, Weimann A, Pichlmayr R. 1997; What constitutes long-term survival after surgery for hilar cholangiocarcinoma? Cancer. 79:26–34. DOI: 10.1002/(SICI)1097-0142(19970101)79:1<26::AID-CNCR5>3.0.CO;2-K. PMID: 8988723.17. Lee SG, Hwang S. 2005; How I do it: assessment of hepatic functional reserve for indication of hepatic resection. J Hepatobiliary Pancreat Surg. 12:38–43. DOI: 10.1007/s00534-004-0949-9. PMID: 15754098.
Article18. Hwang S, Ha TY, Ko GY, Kwon DI, Song GW, Jung DH, et al. 2015; Preoperative sequential portal and hepatic vein embolization in patients with hepatobiliary malignancy. World J Surg. 39:2990–2998. DOI: 10.1007/s00268-015-3194-2. PMID: 26304608.
Article19. Hwang S, Ko GY, Kim MH, Lee SK, Gwon DI, Ha TY, et al. 2016; Preoperative left portal vein embolization for left liver resection in high-risk hepatobiliary malignancy patients. World J Surg. 40:2758–2765. DOI: 10.1007/s00268-016-3618-7. PMID: 27384172.
Article20. Mizumoto R, Kawarada Y, Suzuki H. 1986; Surgical treatment of hilar carcinoma of the bile duct. Surg Gynecol Obstet. 162:153–158. PMID: 3945893.21. Chen XP, Lau WY, Huang ZY, Zhang ZW, Chen YF, Zhang WG, et al. 2009; Extent of liver resection for hilar cholangiocarcinoma. Br J Surg. 96:1167–1175. DOI: 10.1002/bjs.6618. PMID: 19705374.
Article22. Lee SG, Song GW, Hwang S, Ha TY, Moon DB, Jung DH, et al. 2010; Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci. 17:476–489. DOI: 10.1007/s00534-009-0204-5. PMID: 19851704.
Article23. Hwang S, Ha TY, Song GW, Jung DH, Ahn CS, Moon DB, et al. 2015; Quantified risk assessment for major hepatectomy via the indocyanine green clearance rate and liver volumetry combined with standard liver volume. J Gastrointest Surg. 19:1305–1314. DOI: 10.1007/s11605-015-2846-8. PMID: 25947549.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parenchyma-preserving hepatectomy including segments I + IV resection and bile duct resection in a patient with type IV perihilar cholangiocarcinoma: A case report with video clip
- Resection or transplantation for perihilar cholangiocarcinoma
- Surgery for Perihilar Cholangiocarcinoma
- Development of perihilar cholangiocarcinoma at 29 years after first hepatectomy for hepatolithiasis
- Necrosectomy of hepatic left lateral section after blunt abdominal trauma in a patient who underwent central hepatectomy and bile duct resection for perihilar cholangiocarcinoma
