Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2523055
- DOI: http://doi.org/10.14701/ahbps.2021.25.4.509
Abstract
- Obtaining tumor-free resection margins is one of the most important factors for achieving favorable prognosis of patients undergoing resection for hepatobiliary malignancies. In this study, we present our experience of portal vein (PV) wedge resection and patch venoplasty using autologous or homologous vessel grafts for resecting perihilar cholangiocarcinoma, hepatocellular carcinoma, and distal bile duct cancer. Case 1 was 68-year-old male patient with type IV perihilar cholangiocarcinoma who underwent central bisectionectomy with caudate lobectomy and bile duct resection, and PV wedge resection and patch venoplasty with a cryopreserved iliac vein allograft patch. This patient survived 14 months after surgery. Case 2 was 77-year-old male patient with type IIIA perihilar cholangiocarcinoma who underwent left medial sectionectomy with caudate lobectomy, bile duct resection, and PV wedge resection and patch venoplasty with a cryopreserved iliac vein allograft patch. This patient survived 17 months after surgery. Case 3 was 54-year-old male patient with hepatitis B virus-associated liver cirrhosis and hepatocellular carcinoma with PV tumor thrombus who underwent left hepatectomy. The PV wall defect was repaired with an autologous greater saphenous vein patch. This patient survived 11 months after surgery. Case 4 was 65-year-old female patient with distal bile duct cancer who underwent pylorus-preserving pancreaticoduodenectomy, and main PV wedge resection and patch venoplasty with a cryopreserved iliac artery allograft patch. This patient survived 21 months after surgery. In conclusion, PV wedge resection and patch venoplasty can be used to facilitate complete tumor resection in patients undergoing various extents of surgical resection for hepatobiliary malignancies.
Figure
-
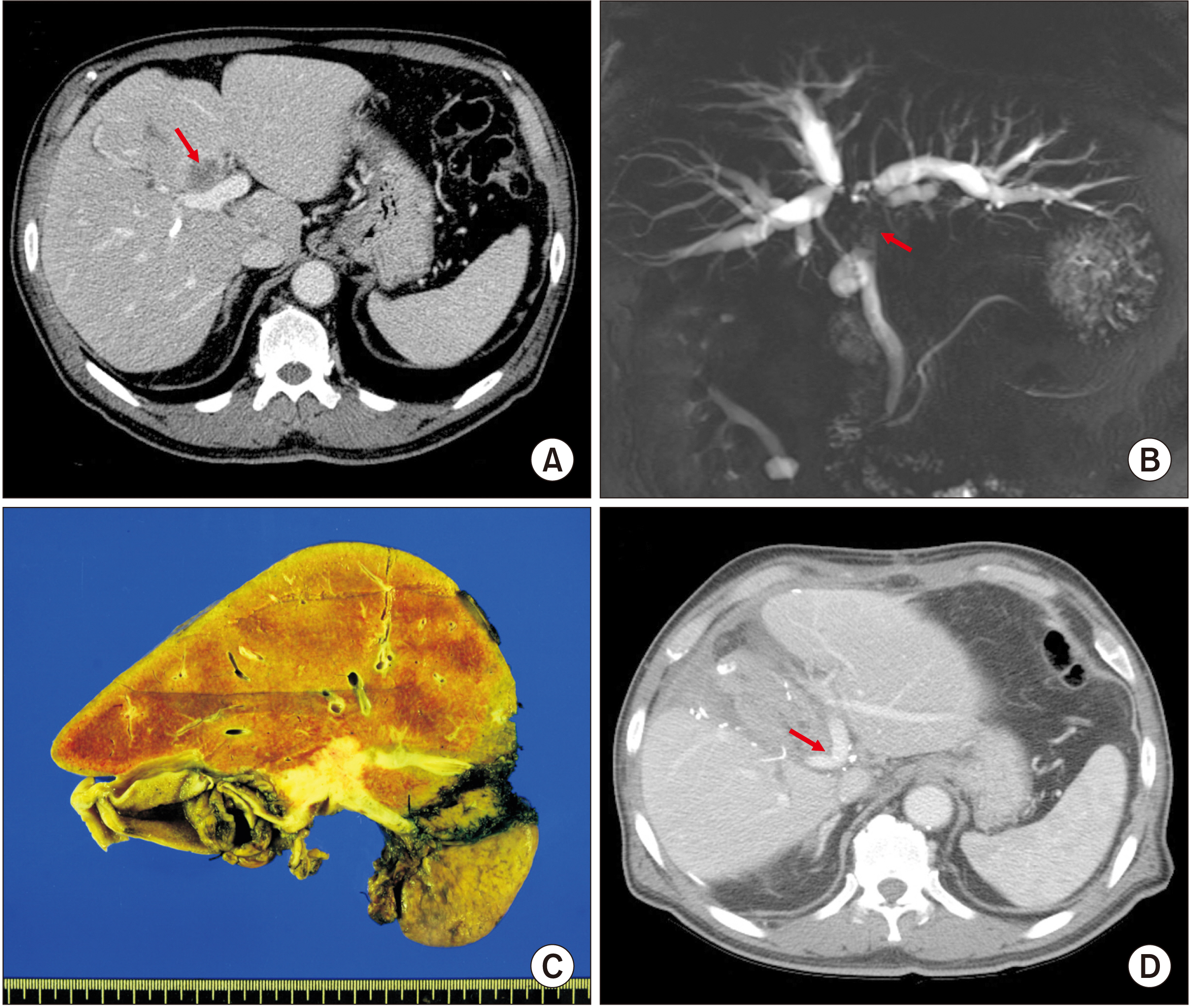
Fig. 1 Perioperative findings of Case 1. (A) Preoperative computed tomography scan shows advanced perihilar cholangiocarcinoma (arrow). (B) Magnetic resonance cholangiopancreatography shows extensive involvement of the hilar bile duct (arrow), indicating Bismuth-Corlette type IV tumor. (C) Gross photograph of the surgical specimen is visible after central bisectionectomy, caudate lobectomy and bile duct resection. (D) Computed tomography scan taken at 2 weeks after surgery shows slightly stenotic portal vein reconstruction site (arrow) at the portal vein confluence portion.

Fig. 2 Intraoperative photographs in Case 1. (A) Tumor invades the confluence portion of the portal vein (PV) bifurcation and the right anterior PV branch (arrow). (B) The invaded PV confluence portion and the right anterior PV branch are elliptically excised and the wall defect is repaired with a cryopreserved iliac vein allograft patch. (C) The roofing patch venoplasty is fully expanded. (D) Central bisectionectomy with caudate lobectomy and bile duct resection are completed.

Fig. 3 Perioperative findings of Case 2. (A, B) Preoperative computed tomography scan shows advanced perihilar cholangiocarcinoma (arrows). (C) Gross photograph of the surgical specimen is visible after left medial sectionectomy, caudate lobectomy and bile duct resection. (D) Computed tomography scan taken at 2 weeks after surgery shows no abnormal findings. B2 and B3 indicate segment II and III ducts, respectively; LHD, left hepatic duct.
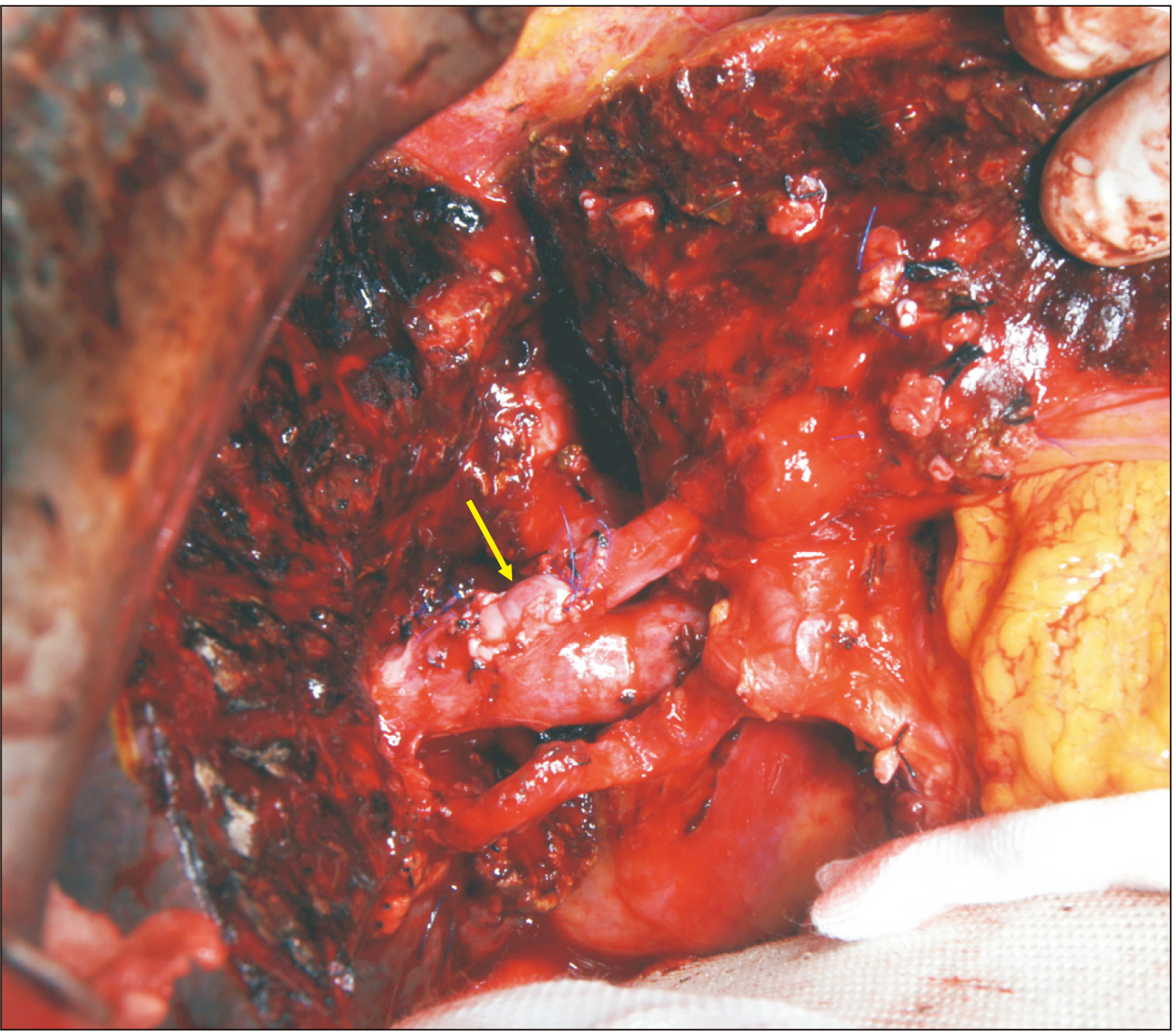
Fig. 4 Intraoperative photographs in Case 2. The tumor-invaded transverse portion of the left portal vein is elliptically excised and the wall defect is repaired with a cryopreserved iliac vein allograft patch (arrow).

Fig. 5 Perioperative findings of Case 3. (A, B) Preoperative computed tomography scan shows hepatocellular carcinoma and portal vein tumor thrombus (arrows) at the left liver. (C) Gross photograph of the surgical specimen is visible after left hepatectomy. (D) Computed tomography scan taken at 1 week after surgery shows no abnormal findings.

Fig. 6 Intraoperative photographs in Case 3. (A) Hepatocellular carcinoma is located at the left liver. (B) The left portal vein is transected at the confluence portion and intraluminal tumor thrombus is visible (arrow). (C, D) The portal vein wall defect is repaired with an autologous greater saphenous vein patch (arrows).
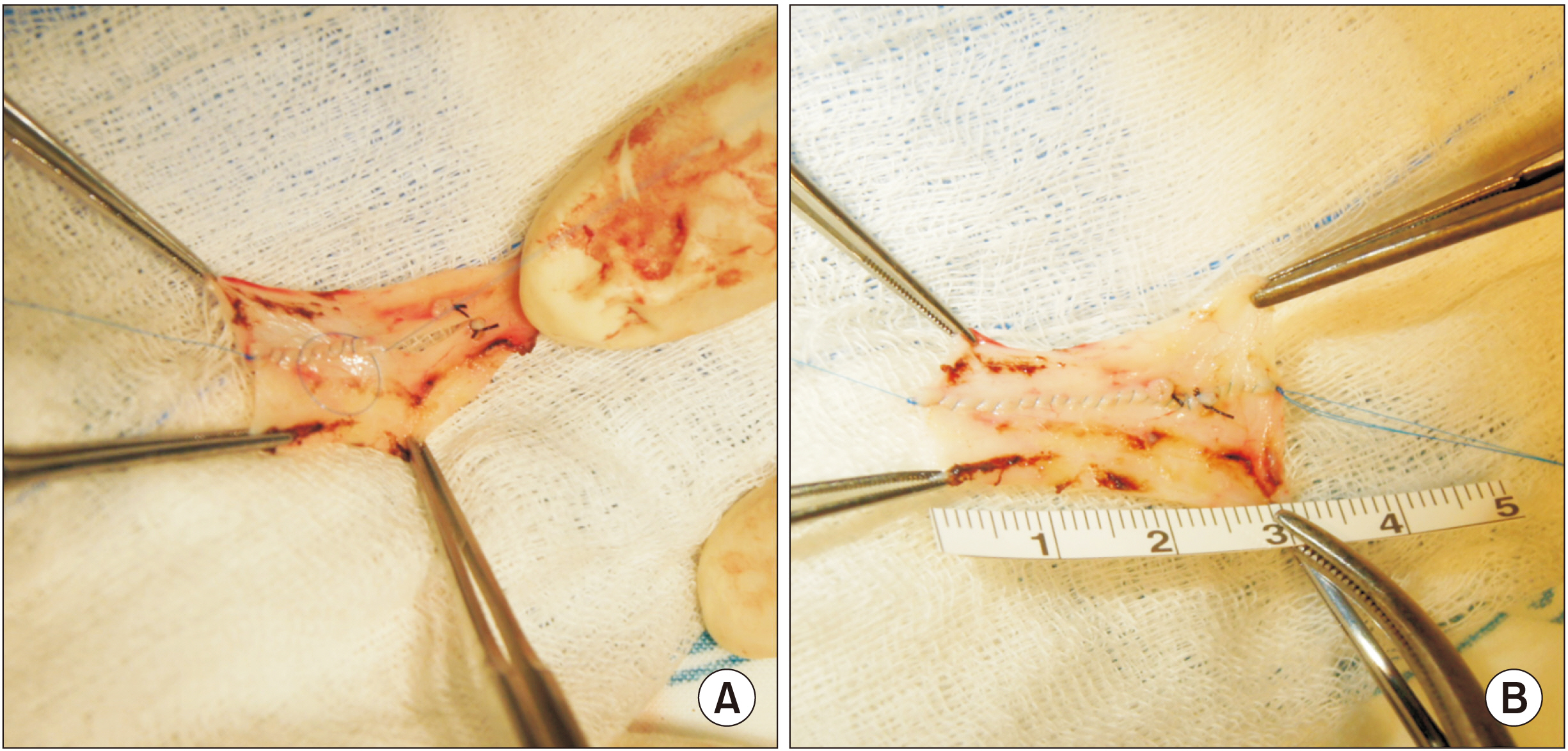
Fig. 7 Intraoperative photographs showing the greater saphenous vein patch in Case 3. Two greater saphenous vein segments are sutured (A) to make a 3 cm × 2 cm-sized rectangular patch (B).

Fig. 8 Perioperative findings of Case 4. (A) Preoperative computed tomography scan shows distal bile duct cancer (arrow). (B) Magnetic resonance cholangiopancreatography shows complete obstruction of the distal bile duct (arrow). (C) Gross photograph of the surgical specimen is visible after pylorus-preserving pancreaticoduodenectomy. (D) Computed tomography scan taken at 3 weeks after surgery shows a long stenosis at the site of portal vein reconstruction proximal to the superior mesenteric vein-splenic vein confluence portion (arrow).

Fig. 9 Intraoperative photographs in Case 4. (A, B) The main portal vein is invaded by the tumor (arrow). A cryopreserved iliac artery allograft is visible. (C, D) The tumor-invaded main portal vein wall is elliptically excised and the wall defect is repaired with a cryopreserved iliac artery allograft patch (arrow).
Reference
-
1. Chen W, Ke K, Chen YL. 2014; Combined portal vein resection in the treatment of hilar cholangiocarcinoma: a systematic review and meta-analysis. Eur J Surg Oncol. 40:489–495. DOI: 10.1016/j.ejso.2014.02.231. PMID: 24685155.
Article2. Wu XS, Dong P, Gu J, Li ML, Wu WG, Lu JH, et al. 2013; Combined portal vein resection for hilar cholangiocarcinoma: a meta-analysis of comparative studies. J Gastrointest Surg. 17:1107–1115. DOI: 10.1007/s11605-013-2202-9. PMID: 23592188.
Article3. Ebata T, Nagino M, Kamiya J, Uesaka K, Nagasaka T, Nimura Y. 2003; Hepatectomy with portal vein resection for hilar cholangiocarcinoma: audit of 52 consecutive cases. Ann Surg. 238:720–727. DOI: 10.1097/01.sla.0000094437.68038.a3. PMID: 14578735. PMCID: PMC1356151.4. Hwang S, Ha TY, Jung DH, Park JI, Lee SG. 2007; Portal vein interposition using homologous iliac vein graft during extensive resection for hilar bile duct cancer. J Gastrointest Surg. 11:888–892. DOI: 10.1007/s11605-007-0146-7. PMID: 17440791.
Article5. Kim SM, Hwang S. 2021; Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: a report of two cases. Ann Hepatobiliary Pancreat Surg. 25:132–138. DOI: 10.14701/ahbps.2021.25.1.132. PMID: 33649266. PMCID: PMC7952668.
Article6. Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK, et al. 2017. AJCC cancer staging manual. 8th ed. Springer;New York: DOI: 10.1007/978-3-319-40618-3.7. Hwang S, Ha TY, Ko GY, Kwon DI, Song GW, Jung DH, et al. 2015; Preoperative sequential portal and hepatic vein embolization in patients with hepatobiliary malignancy. World J Surg. 39:2990–2998. DOI: 10.1007/s00268-015-3194-2. PMID: 26304608.
Article8. Sakamoto Y, Yamamoto J, Saiura A, Koga R, Kokudo N, Kosuge T, et al. 2004; Reconstruction of hepatic or portal veins by use of newly customized great saphenous vein grafts. Langenbecks Arch Surg. 389:110–113. DOI: 10.1007/s00423-003-0452-9. PMID: 15004752.
Article9. Lin CC, Hsieh CE, Chen YL. 2013; Great saphenous vein harvesting for venous outflow reconstruction in living donor liver transplantation - a minimally invasive refinement of the conventional procedure. Int J Surg. 11:249–252. DOI: 10.1016/j.ijsu.2013.01.004. PMID: 23352846.
Article10. Hwang S, Ko GY. 2020; Right trisectionectomy with en bloc portal vein resection for cholangiocarcinoma after preoperative stenting for main portal vein occlusion. Ann Hepatobiliary Pancreat Surg. 24:174–181. DOI: 10.14701/ahbps.2020.24.2.174. PMID: 32457263. PMCID: PMC7271116.
Article11. Namgoong JM, Hwang S, Oh SH, Kim KM, Park GC, Ahn CS, et al. 2020; Living-donor liver transplantation with inferior vena cava replacement in an infant recipient with advanced hepatoblastoma. Ann Hepatobiliary Pancreat Surg. 24:72–77. DOI: 10.14701/ahbps.2020.24.1.72. PMID: 32181433. PMCID: PMC7061035.
Article12. Kwon H, Kwon H, Hong JP, Han Y, Park H, Song GW, et al. 2015; Use of cryopreserved cadaveric arterial allograft as a vascular conduit for peripheral arterial graft infection. Ann Surg Treat Res. 89:51–54. DOI: 10.4174/astr.2015.89.1.51. PMID: 26131446. PMCID: PMC4481033.
Article13. Hwang S, Moon DB, Kim KH, Ahn CS, Song GW, Jung DH, et al. Prognostic accuracy of the ADV score following resection of hepatocellular carcinoma with portal vein tumor thrombosis. J Gastrointest Surg. 2020; https://doi.org/10.1007/s11605-020-04800-6 [in press]. DOI: 10.1007/s11605-020-04800-6. PMID: 32948961.
Article14. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A III. 2010. AJCC cancer staging manual. 7th ed. Springer;New York:15. Maeta T, Ebata T, Hayashi E, Kawahara T, Mizuno S, Matsumoto N, et al. 2017; Pancreatoduodenectomy with portal vein resection for distal cholangiocarcinoma. Br J Surg. 104:1549–1557. DOI: 10.1002/bjs.10596. PMID: 28782798.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
- Usability of cryopreserved homologous great saphenous vein for hepatobiliarypancreatic surgery and living donor liver transplantation
- Clinical applicability of autologous great saphenous vein for living donor liver transplantation
- Reconstruction of portal vein and superior mesenteric vein after extensive resection for pancreatic cancer
- Techniques of Oncovascular Reconstruction of Portal and Mesenteric Veins during Pancreatic and Hepatobiliary Surgery
