Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
- KMID: 2513187
- DOI: http://doi.org/10.14701/ahbps.2021.25.1.132
Abstract
- Margin-free resection is one of the most important factors for favorable prognosis in patients undergoing resection for hepatobiliary malignancies. Herein, we present two cases of hepatobiliary malignancies in patients who underwent bile duct resection combined with hilar portal vein (PV) resection and vein allograft patch plasty. The first case was a 51-year-old female patient with gallbladder cancer, in whom we performed extended cholecystectomy, bile duct resection and extensive lymph node dissection. The tumor-invaded PV wall was meticulously excised and the defect was repaired with a cryopreserved iliac vein allograft patch. The extent of the tumor was pT4N2M0 (stage IVB), thus concurrent chemoradiation therapy and adjuvant chemotherapy were performed. This patient is currently alive for 7 years after surgery without any evidence of tumor recurrence. The second case was a 79-year-old male patient with perihilar cholangiocarcinoma of type I and gallbladder cancer, in whom extended bile duct resection and extensive lymph node dissection were performed. The extent of the bile duct tumor was pT4N1M0 (stage IVA) and that of gallbladder tumor was pT2N0M0 (stage II). No additional treatment was provided because of old age and poor general condition. This patient passed away 11 months after surgery due to rapid progression of tumor recurrence. In conclusion, hilar PV wedge resection and roofing patch venoplasty is a useful option to facilitate complete tumor resection in patients undergoing bile duct resection for hepatobiliary malignancy.
Keyword
Figure
-

Fig. 1 Preoperative radiologic findings of Case No. 1. (A, B) Computed tomography scan shows advanced gallbladder cancer with multiple hepatoduodenal ligament lymph node metastases and invasion of the right posterior portal vein (arrows). (C) Magnetic resonance cholangiopancreatography shows common hepatic duct invasion by the metastatic lymph nodes. (D) Fluorodeoxyglucose- positron emission tomography scan shows gallbladder cancer with multiple lymph node metastasis.
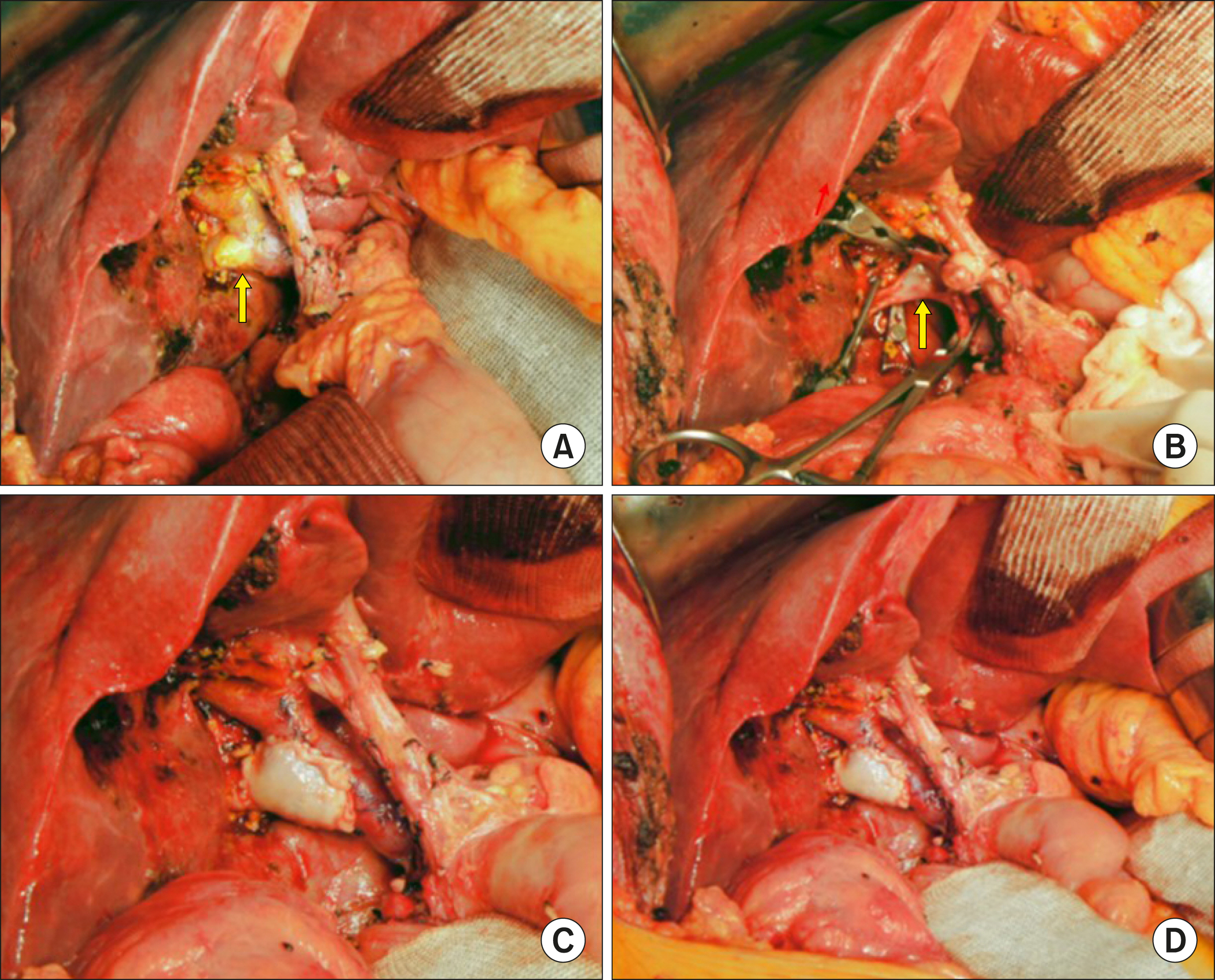
Fig. 2 Intraoperative photographs of wedge resection of the hilar portal vein (PV) invasion and roof patch venoplasty in Case No. 1. (A) The tumor invaded the branching portion of the right posterior section PV (arrow). (B) The invaded PV wall was excised (arrow). (C, D) The defect at the PV wall was repaired with a cryopreserved iliac vein allograft patch.
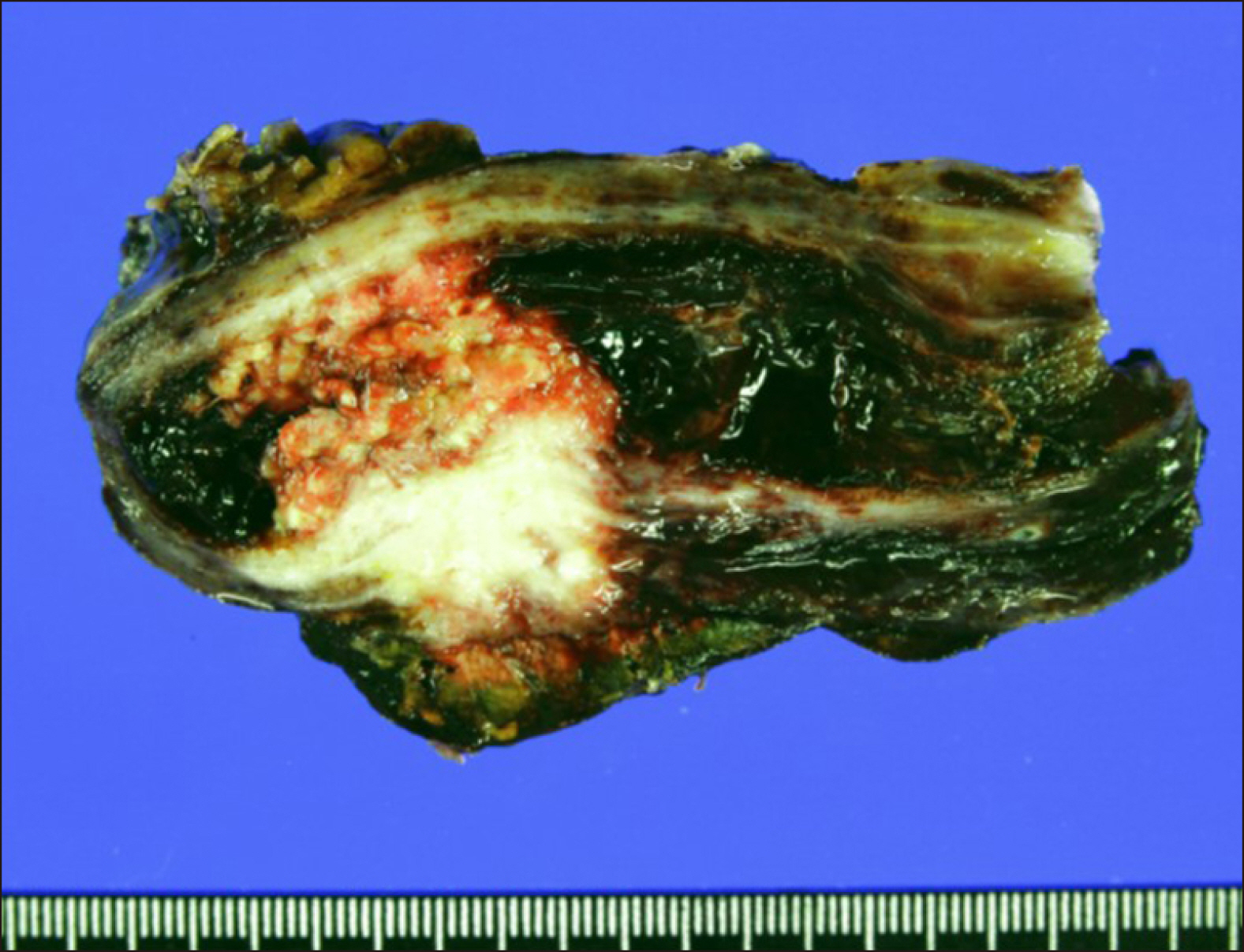
Fig. 3 Gross photographs of Case No. 1 specimen after extended cholecystectomy and bile duct resection showing adenosquamous carcinoma of the gallbladder.
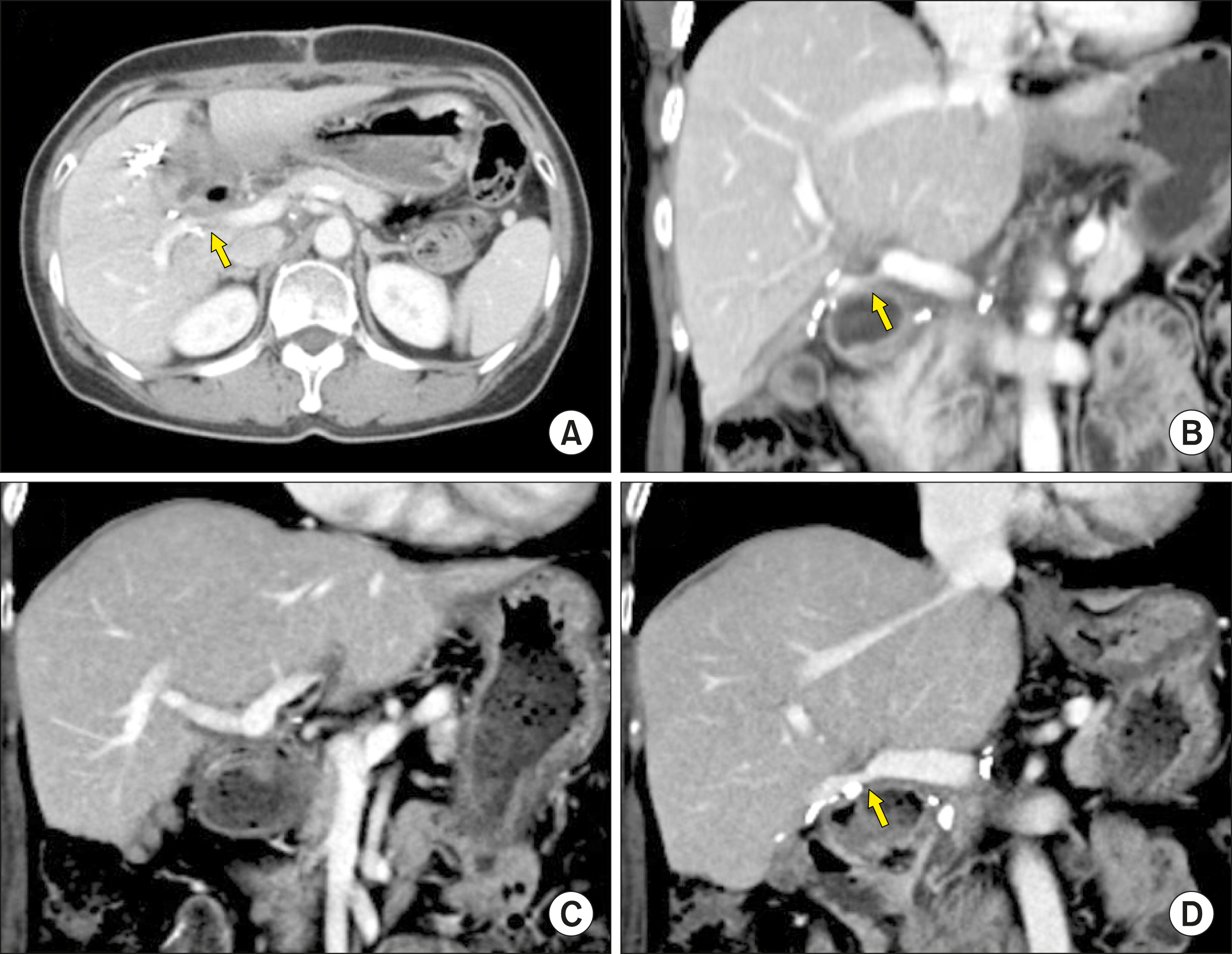
Fig. 4 Follow-up computed tomography scans of Case No. 1 taken at 2 weeks (A, B) and 6 years (C, D) after the operation. The arrows indicate stenosis at the site of portal vein patch venoplasty.

Fig. 5 Preoperative radiologic findings of Case No. 2. (A) Computed tomography scan shows perihilar cholangiocarcinoma of type I (arrow). (B) Magnetic resonance cholangiopancreatography shows the involvement of the hilar bile duct. (C) Fluorodeoxyglucose-positron emission tomography scan shows extrahepatic bile duct cancer. (D) Reconstructed compute tomography image shows the suspected site of portal vein invasion (arrow).
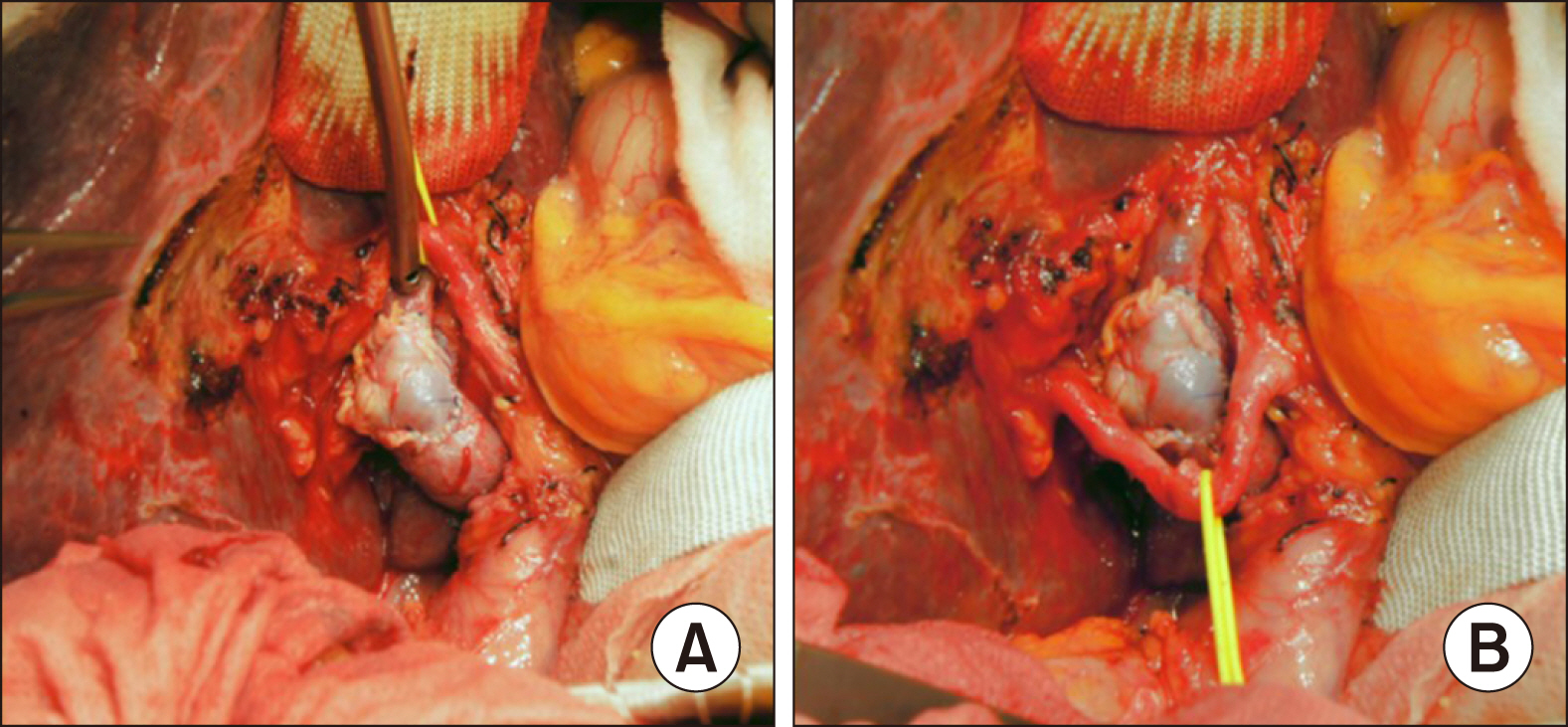
Fig. 6 Intraoperative photographs of the wedge resection of the hilar portal vein (PV) invasion and roof patch venoplasty in Case No. 2. (A) The invaded PV confluence portion is partially excised and repaired with a cryopreserved iliac vein allograft patch. (B) The redundant PV patch is fully expanded.

Fig. 7 Gross photographs of Case No. 2 specimen after bile duct resection showing double primary tumors at the hilar bile duct and gallbladder.
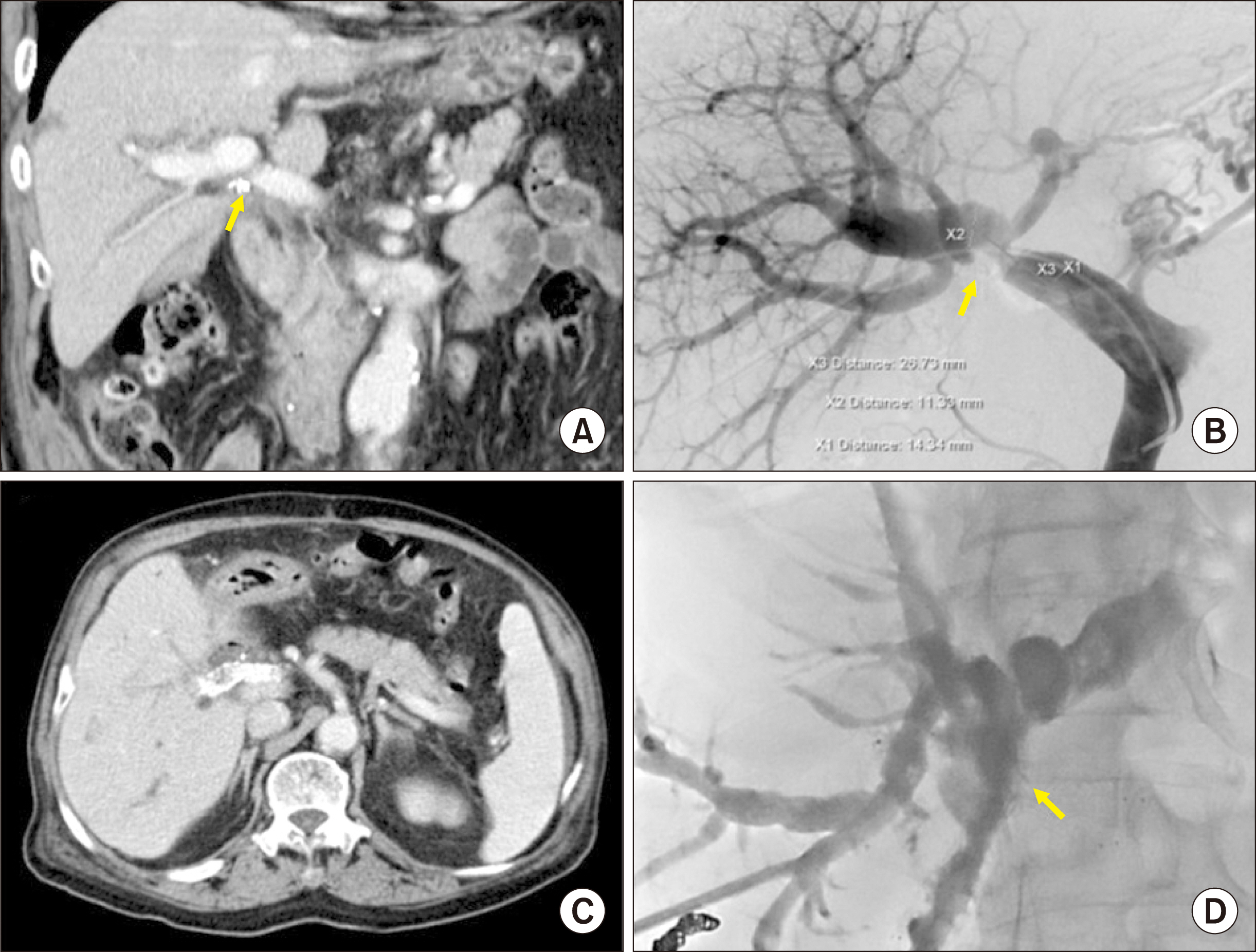
Fig. 8 Follow-up imaging studies of Case No. 2. (A) Computed tomography taken at 4 months shows slight stenosis of the portal vein (PV). (B) At 6 months, the PV resection site is noticeably stenotic, thus percutaneous PV stenting is performed. (C) Computed tomography scan taken at 7 months shows the expansion of the PV stent with focal stenosis. (D) At 8 months, percutaneous biliary stenting is performed to manage tumor recurrence at the hepaticojejunostomy site.
Cited by 1 articles
-
Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
Byeong-Gon Na, Shin Hwang, Dong-Hwan Jung, Sung-Gyu Lee
Ann Hepatobiliary Pancreat Surg. 2021;25(4):509-516. doi: 10.14701/ahbps.2021.25.4.509.
Reference
-
1. Chen W, Ke K, Chen YL. 2014; Combined portal vein resection in the treatment of hilar cholangiocarcinoma: a systematic review and meta-analysis. Eur J Surg Oncol. 40:489–495. DOI: 10.1016/j.ejso.2014.02.231. PMID: 24685155.
Article2. Wu XS, Dong P, Gu J, Li ML, Wu WG, Lu JH, et al. 2013; Combined portal vein resection for hilar cholangiocarcinoma: a meta-analysis of comparative studies. J Gastrointest Surg. 17:1107–1115. DOI: 10.1007/s11605-013-2202-9. PMID: 23592188.
Article3. Ebata T, Nagino M, Kamiya J, Uesaka K, Nagasaka T, Nimura Y. 2003; Hepatectomy with portal vein resection for hilar cholangiocarcinoma: audit of 52 consecutive cases. Ann Surg. 238:720–727. DOI: 10.1097/01.sla.0000094437.68038.a3. PMID: 14578735. PMCID: PMC1356151.4. Sakamoto Y, Yamamoto J, Saiura A, Koga R, Kokudo N, Kosuge T, et al. 2004; Reconstruction of hepatic or portal veins by use of newly customized great saphenous vein grafts. Langenbecks Arch Surg. 389:110–113. DOI: 10.1007/s00423-003-0452-9. PMID: 15004752.
Article5. Lin CC, Hsieh CE, Chen YL. 2013; Great saphenous vein harvesting for venous outflow reconstruction in living donor liver transplantation - a minimally invasive refinement of the conventional procedure. Int J Surg. 11:249–252. DOI: 10.1016/j.ijsu.2013.01.004. PMID: 23352846.
Article6. Hwang S, Sung KB, Park YH, Jung DH, Lee SG. 2007; Portal vein stenting for portal hypertension caused by local recurrence after pancreatoduodenectomy for periampullary cancer. J Gastrointest Surg. 11:333–337. DOI: 10.1007/s11605-006-0058-y. PMID: 17458607.
Article7. Zhou ZQ, Lee JH, Song KB, Hwang JW, Kim SC, Lee YJ, et al. 2014; Clinical usefulness of portal venous stent in hepatobiliary pancreatic cancers. ANZ J Surg. 84:346–352. DOI: 10.1111/ans.12046. PMID: 23421858.
Article8. Mizuno T, Ebata T, Yokoyama Y, Igami T, Sugawara G, Mori Y, et al. 2015; Percutaneous transhepatic portal vein stenting for malignant portal vein stenosis secondary to recurrent perihilar biliary cancer. J Hepatobiliary Pancreat Sci. 22:740–745. DOI: 10.1002/jhbp.265. PMID: 26084448.
Article9. Hwang S, Ha TY, Jung DH, Park JI, Lee SG. 2007; Portal vein interposition using homologous iliac vein graft during extensive resection for hilar bile duct cancer. J Gastrointest Surg. 11:888–892. DOI: 10.1007/s11605-007-0146-7. PMID: 17440791.
Article10. Hwang S, Ko GY. 2020; Right trisectionectomy with en bloc portal vein resection for cholangiocarcinoma after preoperative stenting for main portal vein occlusion. Ann Hepatobiliary Pancreat Surg. 24:174–181. DOI: 10.14701/ahbps.2020.24.2.174. PMID: 32457263. PMCID: PMC7271116.
Article11. Namgoong JM, Hwang S, Oh SH, Kim KM, Park GC, Ahn CS, et al. 2020; Living-donor liver transplantation with inferior vena cava replacement in an infant recipient with advanced hepatoblastoma. Ann Hepatobiliary Pancreat Surg. 24:72–77. DOI: 10.14701/ahbps.2020.24.1.72. PMID: 32181433. PMCID: PMC7061035.
Article12. Kwon H, Kwon H, Hong JP, Han Y, Park H, Song GW, et al. 2015; Use of cryopreserved cadaveric arterial allograft as a vascular conduit for peripheral arterial graft infection. Ann Surg Treat Res. 89:51–54. DOI: 10.4174/astr.2015.89.1.51. PMID: 26131446. PMCID: PMC4481033.
Article13. Hwang S, Ha TY, Song GW, Jung DH. 2016; Cluster hepaticojejunostomy with radial spreading anchoring traction technique for secure reconstruction of widely opened hilar bile ducts. Korean J Hepatobiliary Pancreat Surg. 20:66–70. DOI: 10.14701/kjhbps.2016.20.2.66. PMID: 27212993. PMCID: PMC4874047.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
- Standard and modified techniques for parenchyma-preserving hepatectomy focused on segments I+IV resection in patients with perihilar cholangiocarcinoma
- Successful laparoscopic living donor right hepatectomy in a case with challenging portal vein variation
- A potential intraoperative disaster averted: Preduodenal portal vein compressing a preduodenal common bile duct
- Long-term Result of Radical Resection for Hilar Bile Duct Cancer
