Current Anticoagulant Usage Patterns and Determinants in Korean Patients with Nonvalvular Atrial Fibrillation
- Ha HS

- Kim J
- Lee YS
- Kim TH
- Lee JM
- Park J
- Park JK
- Kang KW
- Shim J
- Uhm JS
- Park HW
- Cha MJ
- Choi EK
- Kim J
- Kim JB
- Kim C
- Joung B
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. cby6908@yuhs.ac
- 2Division of Cardiology, Department of Internal Medicine, Daegu Catholic University Medical Center, Daegu, Korea.
- 3Division of Cardiology, Department of Internal Medicine, Kyung Hee University Hospital, School of Medicine, Kyung Hee University, Seoul, Korea.
- 4Department of Cardiology, School of Medicine, Ewha Womans University, Seoul, Korea.
- 5Department of Cardiology, Hanyang University Seoul Hospital, Seoul, Korea.
- 6Division of Cardiology, Eulji University Hospital, Daejeon, Korea.
- 7Division of Cardiology, Department of Internal Medicine, Korea University Medical Center, Seoul, Korea.
- 8Department of Cardiology, Chonnam National University Hospital, Chonnam National University School of Medicine, Gwangju, Korea.
- 9Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 10Heart Institute, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 11Department of Preventive Medicine, Institute of Human Complexity and Systems Science, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2468486
- DOI: http://doi.org/10.3349/ymj.2020.61.2.120
Abstract
- PURPOSE
Stroke prevention in patients with atrial fibrillation (AF) is influenced by many factors. Using a contemporary registry, we evaluated variables associated with the use of warfarin or direct oral anticoagulants (OACs).
MATERIALS AND METHODS
In the prospective multicenter CODE-AF registry, 10529 patients with AF were evaluated. Multivariate analyses were performed to identify variables associated with the use of anticoagulants.
RESULTS
The mean age of the patients was 66.9±14.4 years, and 64.9% were men. The mean CHA2DS2-VASc and HAS-BLED scores were 2.6±1.7 and 1.8±1.1, respectively. In patients with high stroke risk (CHA2DS2-VASc ≥2), OACs were used in 83.2%, including direct OAC in 68.8%. The most important factors for non-OAC treatment were end-stage renal disease [odds ratio (OR) 0.27; 95% confidence interval (CI): 0.19-0.40], myocardial infarct (OR 0.53; 95% CI: 0.40-0.72), and major bleeding (OR 0.57; 95% CI: 0.39-0.84). Female sex (OR 1.40; 95% CI: 1.21-1.61), cancer (OR 1.78; 95% CI: 1.38-2.29), and smoking (OR 1.60; 95% CI: 1.15-2.24) were factors favoring direct OAC use over warfarin. Among patients receiving OACs, the rate of combined antiplatelet agents was 7.8%. However, 73.6% of patients did not have any indication for a combination of antiplatelet agents.
CONCLUSION
Renal disease and history of valvular heart disease were associated with warfarin use, while cancer and smoking status were associated with direct OAC use in high stroke risk patients. The combination of antiplatelet agents with OAC was prescribed in 73.6% of patients without definite indications recommended by guidelines.
Keyword
MeSH Terms
Figure
-
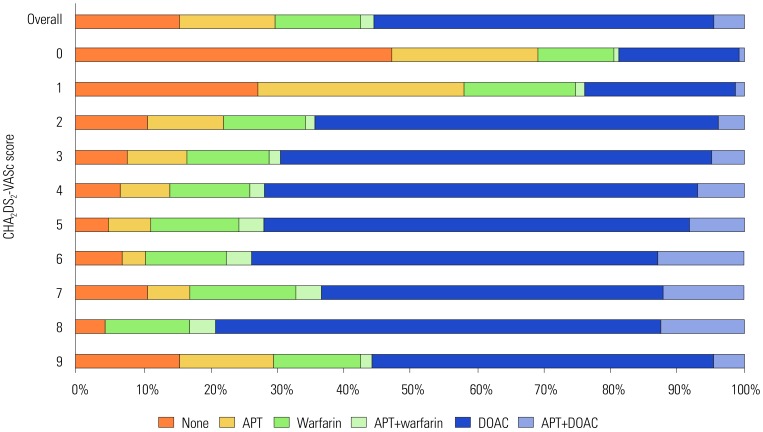
Fig. 1 Method of stroke prevention in patients with AF according to CHA2DS2-VASc score. AF, atrial fibrillation; APT, antiplatelet therapy; DOAC, direct oral anticoagulant.
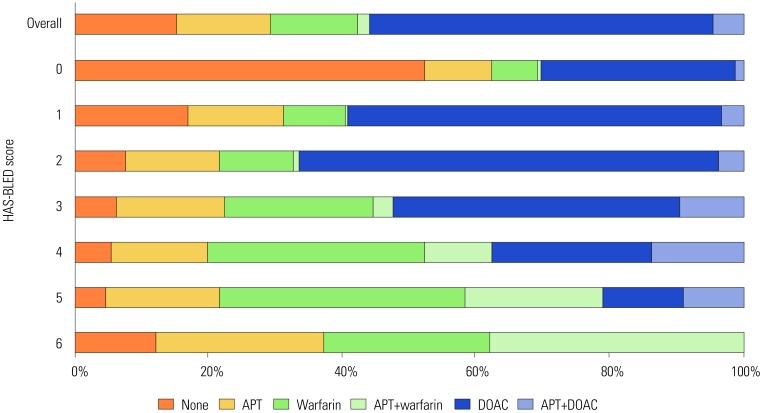
Fig. 2 Method of stroke prevention in patients with AF according to HAS-BLED score. AF, atrial fibrillation; APT, antiplatelet therapy; DOAC, direct oral anticoagulant.
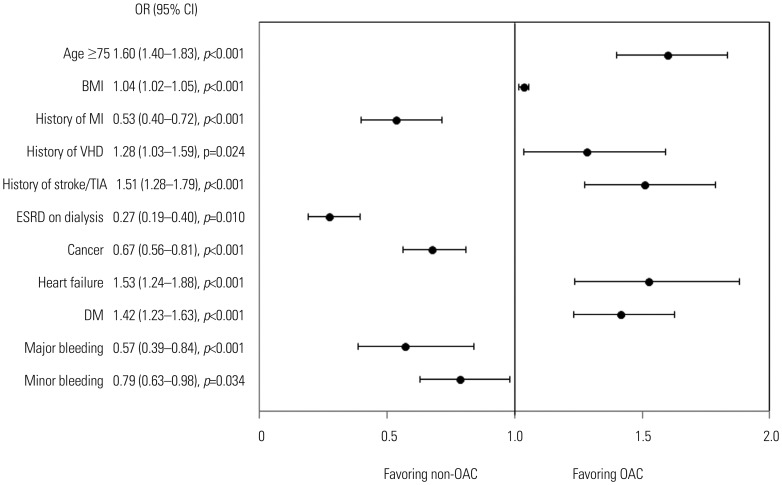
Fig. 3 Factors favoring OAC or non-OAC treatment in patients with CHA2DS2-VASc ≥2. OAC, oral anticoagulant; BMI, body mass index; MI, myocardial infarct; VHD, valvular heart disease; TIA, transient ischemic attack; ESRD, end-stage renal disease; DM, diabetes mellitus; OR, odds ratio; CI, confidence interval.
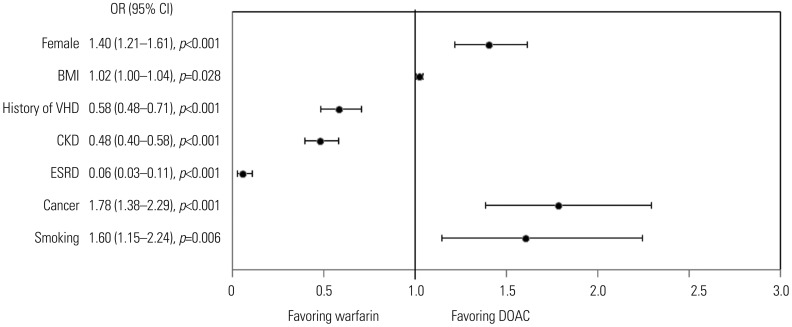
Fig. 4 Factors favoring warfarin or DOAC in patients with CHA2DS2-VASc ≥2. DOAC, direct oral anticoagulant; BMI, body mass index; VHD, valvular heart disease; CKD, chronic kidney disease; ESRD, end-stage renal disease; OR, odds ratio; CI, confidence interval.
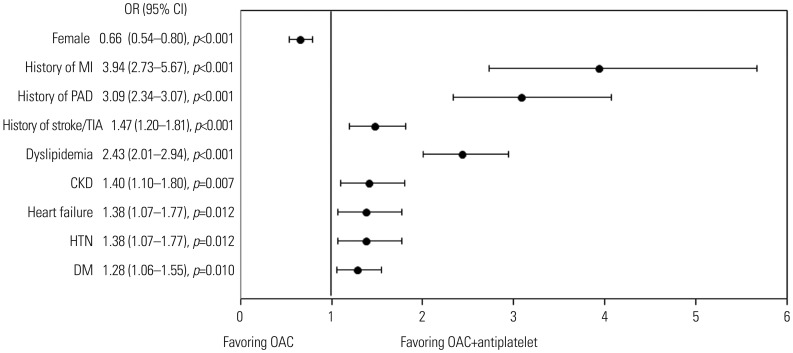
Fig. 5 Factors favoring OAC plus antiplatelet in patients with CHA2DS2-VASc ≥2. OAC, oral anticoagulant; MI, myocardial infarct; PAD, peripheral arterial disease; TIA, transient ischemic attack; CKD, chronic kidney disease; HTN, hypertension; DM, diabetes mellitus; OR, odds ratio; CI, confidence interval.
Reference
-
1. Lee H, Kim TH, Baek YS, Uhm JS, Pak HN, Lee MH, et al. The trends of atrial fibrillation-related hospital visit and cost, treatment pattern and mortality in Korea: 10-year nationwide sample cohort data. Korean Circ J. 2017; 47:56–64. PMID: 28154592.
Article2. Kim TH, Yang PS, Uhm JS, Kim JY, Pak HN, Lee MH, et al. CHA2DS2-VASc score (congestive heart failure, hypertension, age ≥75 [doubled], diabetes mellitus, prior stroke or transient ischemic attack [doubled], vascular disease, age 65-74, female) for stroke in Asian patients with atrial fibrillation: a Korean nationwide sample cohort study. Stroke. 2017; 48:1524–1530. PMID: 28455320.3. Kim D, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. 2018; 202:20–26. PMID: 29802976.
Article4. Kim D, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. Increasing trends in hospital care burden of atrial fibrillation in Korea, 2006 through 2015. Heart. 2018; 104:2010–2017. PMID: 29666179.
Article5. Joung B, Lee JM, Lee KH, Kim TH, Choi EK, Lim WH, et al. 2018 Korean guideline of atrial fibrillation management. Korean Circ J. 2018; 48:1033–1080. PMID: 30403013.
Article6. Yoon M, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. Dynamic changes of CHA2DS2-VASc score and the risk of ischaemic stroke in Asian patients with atrial fibrillation: a nationwide cohort study. Thromb Haemost. 2018; 118:1296–1304. PMID: 29723875.
Article7. Kim KE, Yang PS, Jang E, Kim S, Joung B. Antithrombotic medication and the risk of vitreous hemorrhage in atrial fibrillation: Korean National Health Insurance Service National Cohort. Yonsei Med J. 2019; 60:65–72. PMID: 30554492.
Article8. Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007; 146:857–867. PMID: 17577005.
Article9. van Walraven C, Hart RG, Singer DE, Laupacis A, Connolly S, Petersen P, et al. Oral anticoagulants vs aspirin in nonvalvular atrial fibrillation: an individual patient meta-analysis. JAMA. 2002; 288:2441–2448. PMID: 12435257.10. Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009; 361:1139–1151. PMID: 19717844.
Article11. Lee SR, Lee YS, Park JS, Cha MJ, Kim TH, Park J, et al. Label adherence for non-vitamin K antagonist oral anticoagulants in a prospective cohort of Asian patients with atrial fibrillation. Yonsei Med J. 2019; 60:277–284. PMID: 30799590.
Article12. Nelson WW, Song X, Coleman CI, Thomson E, Smith DM, Damaraju CV, et al. Medication persistence and discontinuation of rivaroxaban versus warfarin among patients with non-valvular atrial fibrillation. Curr Med Res Opin. 2014; 30:2461–2469. PMID: 24926732.
Article13. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37:2893–2962. PMID: 27567408.
Article14. Steffel J, Verhamme P, Potpara TS, Albaladejo P, Antz M, Desteghe L, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation: executive summary. Europace. 2018; 20:1231–1242. PMID: 29562331.
Article15. Lip GYH, Collet JP, Haude M, Byrne R, Chung EH, Fauchier L, et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions: a joint consensus document of the European Heart Rhythm Association (EHRA), European Society of Cardiology Working Group on Thrombosis, European Association of Percutaneous Cardiovascular Interventions (EAPCI), and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS), Latin America Heart Rhythm Society (LAHRS), and Cardiac Arrhythmia Society of Southern Africa (CASSA). Europace. 2019; 21:192–193. PMID: 30052888.
Article16. Lip GY, Windecker S, Huber K, Kirchhof P, Marin F, Ten Berg JM, et al. Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on Thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS). Eur Heart J. 2014; 35:3155–3179. PMID: 25154388.17. Kim H, Kim TH, Cha MJ, Lee JM, Park J, Park JK, et al. A prospective survey of atrial fibrillation management for real-world guideline adherence: COmparison study of Drugs for symptom control and complication prEvention of Atrial Fibrillation (CODE-AF) Registry. Korean Circ J. 2017; 47:877–887. PMID: 29171211.
Article18. January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC Jr, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014; 130:2071–2104. PMID: 24682348.
Article19. SayXMLLink_XYZn B, Okutucu S, Yılmaz MB, Özdemir K, Aydınlar A, S¸ahin DY, et al. Antithrombotic treatment patterns and stroke prevention in patients with atrial fibrillation in TURKEY: inferences from GARFIELD-AF registry. Anatol J Cardiol. 2019; 21:272–280. PMID: 31062761.
Article20. Olesen JB, Sørensen R, Hansen ML, Lamberts M, Weeke P, Mikkelsen AP, et al. Non-vitamin K antagonist oral anticoagulation agents in anticoagulant naïve atrial fibrillation patients: Danish nationwide descriptive data 2011-2013. Europace. 2015; 17:187–193. PMID: 25236181.21. Moreno-Arribas J, Bertomeu-González V, Anguita-Sanchez M, Cequier Á, Muñiz J, Castillo J, et al. Choice of new oral anticoagulant agents versus vitamin K antagonists in atrial fibrillation: FANTASIIA Study. J Cardiovasc Pharmacol Ther. 2016; 21:150–156. PMID: 26229096.22. Lauffenburger JC, Farley JF, Gehi AK, Rhoney DH, Brookhart MA, Fang G. Factors driving anticoagulant selection in patients with atrial fibrillation in the United States. Am J Cardiol. 2015; 115:1095–1101. PMID: 25724781.
Article23. Camm AJ, Lip GY, De Caterina R, Savelieva I, Atar D, Hohnloser SH, et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation--developed with the special contribution of the European Heart Rhythm Association. Europace. 2012; 14:1385–1413. PMID: 22923145.24. Jung H, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation with hypertrophic cardiomyopathy: a nationwide cohort study. Chest. 2019; 155:354–363. PMID: 30472021.25. Verhoef TI, Redekop WK, Hasrat F, de Boer A, Maitland-van der Zee AH. Cost effectiveness of new oral anticoagulants for stroke prevention in patients with atrial fibrillation in two different European healthcare settings. Am J Cardiovasc Drugs. 2014; 14:451–462. PMID: 25326294.
Article26. Sandhu RK, Bakal JA, Ezekowitz JA, McAlister FA. Risk stratification schemes, anticoagulation use and outcomes: the risk--treatment paradox in patients with newly diagnosed non-valvular atrial fibrillation. Heart. 2011; 97:2046–2050. PMID: 22076011.
Article27. Bernard A, Fauchier L, Pellegrin C, Clementy N, Saint Etienne C, Banerjee A, et al. Anticoagulation in patients with atrial fibrillation undergoing coronary stent implantation. Thromb Haemost. 2013; 110:560–568. PMID: 23846210.
Article28. Azoulay L, Dell’Aniello S, Simon T, Renoux C, Suissa S. The concurrent use of antithrombotic therapies and the risk of bleeding in patients with atrial fibrillation. Thromb Haemost. 2013; 109:431–439. PMID: 23306435.
Article29. Cannon CP, Bhatt DL, Oldgren J, Lip GYH, Ellis SG, Kimura T, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. N Engl J Med. 2017; 377:1513–1524. PMID: 28844193.
Article30. Lopes RD, Heizer G, Aronson R, Vora AN, Massaro T, Mehran R, et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. N Engl J Med. 2019; 380:1509–1524. PMID: 30883055.
Article31. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS Guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019; 74:104–132. PMID: 30703431.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Erratum to “Current Anticoagulant Usage Patterns and Determinants in Korean Patients with Nonvalvular Atrial Fibrillation” by Ha HS, et al. (Yonsei Med J 2020;61(2):120-128.)
- Application of New Oral Anticoagulants: Prevention of Stroke in Patients with Nonvalvular Atrial Fibrillation
- Antithrombotic Therapy for Patients with Nonvalvular Atrial Fibrillation
- Hemoptysis in Quadriplegia with Atrial Fibrillation Who Was Taking Edoxaban: a Case Report
- A Comparative Study on Cerebral Infarction in Patient with Nonvalvular and Valvular Atrial Fibrillation
