World J Mens Health.
2020 Jan;38(1):132-136. 10.5534/wjmh.180130.
Testosterone Replacement Therapy for Patients with Hypogonadism after High Dose-Rate Brachytherapy for High-Risk Prostate Cancer: A Report of Six Cases and Literature Review
- Affiliations
-
- 1Department of Integrative Cancer Therapy and Urology, Kanazawa University Graduate School of Medical Science, Kanazawa, Japan. kshigehara0415@yahoo.co.jp
- KMID: 2465418
- DOI: http://doi.org/10.5534/wjmh.180130
Abstract
- We had six cases of patients who were treated with long-term testosterone replacement therapy (TRT) after high dose-rate (HDR) brachytherapy and androgen deprivation therapy for high-risk prostate cancer. All patients were given testosterone enanthate by intramuscular injection every 3 to 4 weeks. Blood biochemistry including prostate specific antigen (PSA) level was evaluated every 3 to 6 months after TRT, and radiological imaging was performed every 12 months. All patients had slight increases in PSA within the normal range and not indicative of biochemical recurrence. A sudden increase in PSA was observed in one patient, but it finally decreased. Aging male symptoms scale and various metabolic factors were improved by TRT in all of cases. Although adverse events included polycythemia in one patient, no patients experienced disease recurrence or progression during TRT. Our results suggest TRT for high risk-patients with HDR brachytherapy for prostate cancer may be beneficial and safe.
Keyword
MeSH Terms
Figure
-
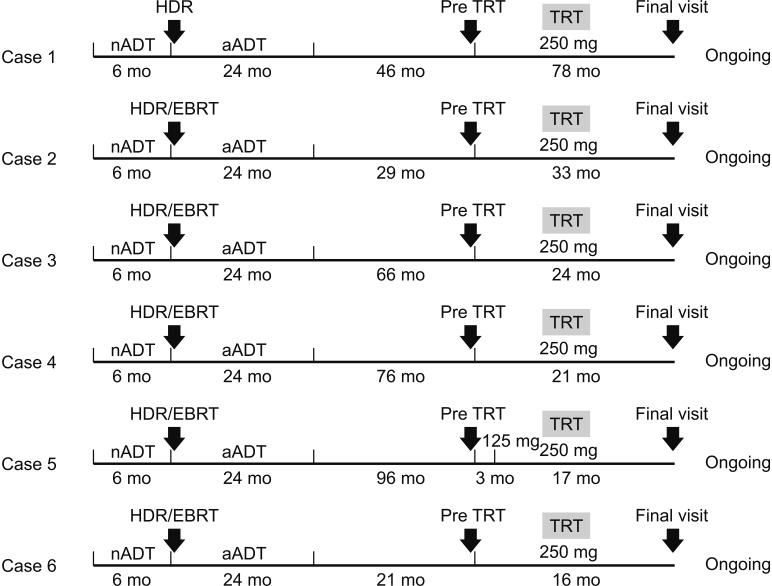
Fig. 1 A flow chart to indicate details in each case, including schedule of therapy, the duration of TRT therapy, follow-up time points and evaluation at each time points. nADT: neoadjuvant androgen deprivation therapy, aADT: adjuvant androgen deprivation therapy, HDR: high dose-rate brachytherapy, TRT: testosterone replacement therapy, EBRT: external beam radiation therapy.
Reference
-
1. Tsujimura A. The relationship between testosterone deficiency and men’s health. World J Mens Health. 2013; 31:126–135. PMID: 24044107.
Article2. Blaya R, Thomaz LD, Guilhermano F, Paludo Ade O, Rhoden L, Halmenschlager G, et al. Total testosterone levels are correlated to metabolic syndrome components. Aging Male. 2016; 19:85–89. PMID: 26961662.
Article3. Kaufman JM, Graydon RJ. Androgen replacement after curative radical prostatectomy for prostate cancer in hypogonadal men. J Urol. 2004; 172:920–922. PMID: 15310998.
Article4. Khera M, Grober ED, Najari B, Colen JS, Mohamed O, Lamb DJ, et al. Testosterone replacement therapy following radical prostatectomy. J Sex Med. 2009; 6:1165–1170. PMID: 19207277.
Article5. Balbontin FG, Moreno SA, Bley E, Chacon R, Silva A, Morgentaler A. Long-acting testosterone injections for treatment of testosterone deficiency after brachytherapy for prostate cancer. BJU Int. 2014; 114:125–130. PMID: 25101359.
Article6. Sarosdy MF. Testosterone replacement for hypogonadism after treatment of early prostate cancer with brachytherapy. Cancer. 2007; 109:536–541. PMID: 17183557.
Article7. Pastuszak AW, Pearlman AM, Lai WS, Godoy G, Sathyamoorthy K, Liu JS, et al. Testosterone replacement therapy in patients with prostate cancer after radical prostatectomy. J Urol. 2013; 190:639–644. PMID: 23395803.
Article8. Pastuszak AW, Khanna A, Badhiwala N, Morgentaler A, Hult M, Conners WP, et al. Testosterone therapy after radiation therapy for low, intermediate and high risk prostate cancer. J Urol. 2015; 194:1271–1276. PMID: 26025500.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Testosterone Replacement Therapy and Prostate Cancer Incidence
- Shifting the Paradigm of Testosterone Replacement Therapy in Prostate Cancer
- Testosterone therapy in men with testosterone deficiency: Are we beyond the point of no return?
- Questioning the evidence behind the Saturation Model for testosterone replacement therapy in prostate cancer
- Current Status of Brachytherapy for Prostate Cancer
