Arch Hand Microsurg.
2019 Dec;24(4):330-334. 10.12790/ahm.2019.24.4.330.
Multiple Bony Mallet on the Same Hand
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Gwangmyeong Sungae Hospital, Gwangmyeong, Korea. psczero@gmail.com
- 2New Hand Hostpital, Daejeon, Korea.
- KMID: 2464468
- DOI: http://doi.org/10.12790/ahm.2019.24.4.330
Abstract
- Mallet finger is a very common finger disease. However, it is very rare for mallet fingers to occur simultaneously on three fingers of the same hand. We report a case of mallet fingers in a 46-year-old female who sustained a fall during a running race. She was injured on the middle, ring, and little fingers. Radiographically, bone fragments were observed on the dorsal side of the distal phalanx base on the middle, ring, and little fingers. She underwent surgical treatment using the extension block method. Extension lag was observed in the fingers other than the little finger (middle finger: 5°, ring finger: 10°). However, evaluation using Crawford's classification revealed good results. Thus, provide data on the treatment of multiple mallet fingers on the same hand.
Keyword
MeSH Terms
Figure
-

Fig. 1 A 46-year-old female with multiple bony mallet on the middle, ring, and little fingers. In each of the fingers, gap between the distal phalanx and the bone fragment are seen (white arrows).
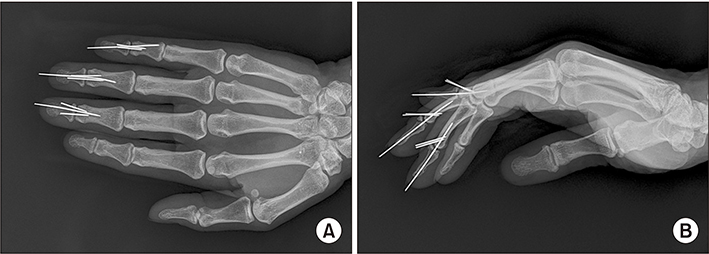
Fig. 2 Immediate postoperative radiologic image: extension block method used in all fingers. (A) Anterioposterior view. (B) Lateral view.
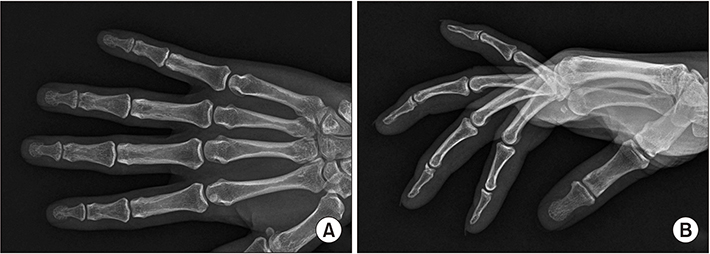
Fig. 3 Follow-up radiologic image 7 months after surgery: bone union with attachment of bone fragment seen. (A) Anterioposterior view. (B) Lateral view.
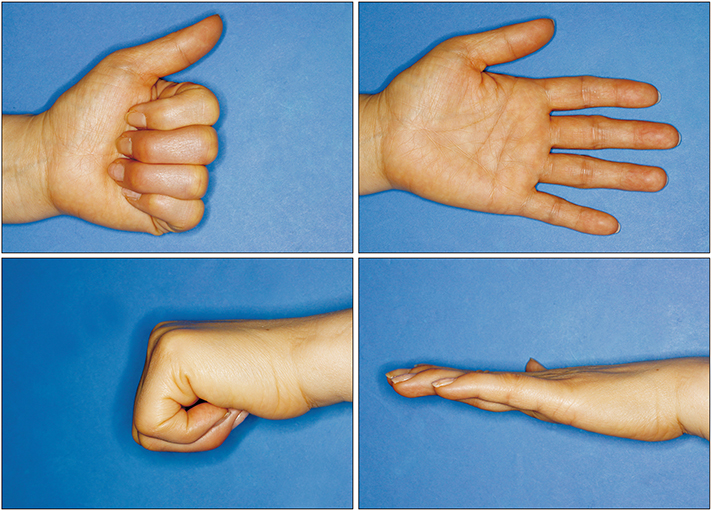
Fig. 4 Six months after operation image. Minimal extension lag (5°–10°) was found.
Reference
-
1. Alla SR, Deal ND, Dempsey IJ. Current concepts: mallet finger. Hand (N Y). 2014; 9:138–144.
Article2. Salazar Botero S, Hidalgo Diaz JJ, Benaïda A, Collon S, Facca S, Liverneaux PA. Review of acute traumatic closed mallet finger injuries in adults. Arch Plast Surg. 2016; 43:134–144.
Article3. Degreef I, De Smet L. Multiple simultaneous mallet fingers in goalkeeper. Hand Surg. 2009; 14:143–144.
Article4. Crawford GP. The molded polythene splint for mallet finger deformities. J Hand Surg Am. 1984; 9:231–237.
Article5. Gurnani N, Hoogendoorn J, Rhemrev S. [Mallet finger: surgery versus splinting]. Ned Tijdschr Geneeskd. 2014; 158:A6941. Dutch.6. Richards SD, Kumar G, Booth S, Naqui SZ, Murali SR. A model for the conservative management of mallet finger. J Hand Surg Br. 2004; 29:61–63.
Article7. Ishiguro T, Itoh Y, Yabe Y, Hashizume N. Extension block with Kirschner wire for fracture dislocation of the distal interphalangeal joint. Tech Hand Up Extrem Surg. 1997; 1:95–102.
Article8. Pegoli L, Toh S, Arai K, Fukuda A, Nishikawa S, Vallejo IG. The Ishiguro extension block technique for the treatment of mallet finger fracture: indications and clinical results. J Hand Surg Br. 2003; 28:15–17.9. Han HH, Cho HJ, Kim SY, Oh DY. Extension block and direct pinning methods for mallet fracture: a comparative study. Arch Plast Surg. 2018; 45:351–356.
Article10. Kim JY, Lee SH. Factors related to distal interphalangeal joint extension loss after extension block pinning of mallet finger fractures. J Hand Surg Am. 2016; 41:414–419.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Physical Therapy-Induced Secondary Bony Mallet Finger Deformity
- Modified Extension Block Technique Using Conjoined Kirschner Wires for Bony Mallet Fingers
- Current concepts in traumatic mallet finger management
- Prognostic Factors of the Extension Block Technique for the Bony Mallet Finger
- Comparison of Surgical Outcomes of Percutaneous K-Wire Fixation in Bony Mallet Fingers with Use of Towel Clip versus 18-Gauge Needle
