Prognostic Factors of the Extension Block Technique for the Bony Mallet Finger
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University College of Medicine, Seoul, Korea. yrchoi@yuhs.ac
- KMID: 2185580
- DOI: http://doi.org/10.4055/jkoa.2010.45.2.127
Abstract
- PURPOSE
The purpose of this study was to evaluate the clinical results and prognostic factors of the extension block technique for treating a bony mallet finger.
MATERIALS AND METHODS
Between July 2002 and January 2009, forty-nine patients who underwent the extension block technique for a bony mallet finger were evaluated. The minimum period of follow up was 6 months. The type of fracture was classified by the Wehbe and Schneider method. The results were evaluated by the Crawford classification. The prognostic factors were analyzed according to age, gender, the timing of the surgery, the mallet fragment angle and the residual displacement.
RESULTS
According the Crawford classification, there were 22 excellent, 20 good, 6 fair and 1 poor results. The poor prognostic factors were an older patient age, subluxation, a smaller mallet fragment angle and smaller postoperative displacement (p<0.05).
CONCLUSION
The prognostic factors of the extension block technique for bony mallet finger were the patient age, subluxation, the mallet fragment angle (more than 30 degrees) and the postoperative displacement.
Figure
-
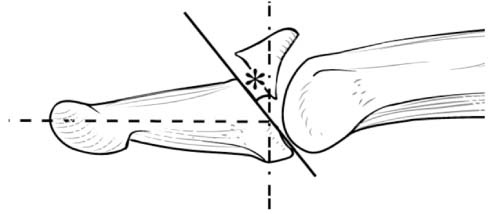
Figure 1 Mallet fragment angle. *Mallet fragment angle (°)=90°-{An acute angle between an axis of distal phalanx (dotted line) and a line of fracture (solid line)}.
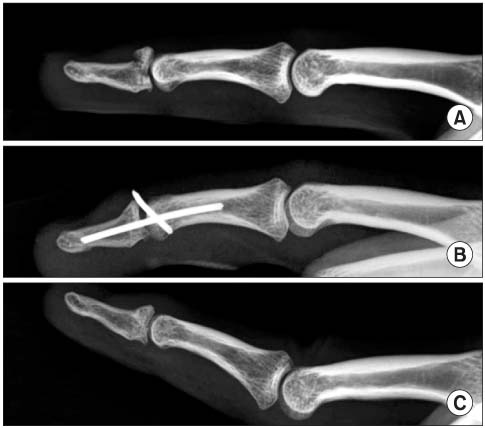
Figure 2 Lateral radiograph of right 3rd finger. (A) Four days ago, a 37-year-old male patient had an injury on his right 3rd finger. Preoperative radiograph showed 70 percents of joint involvement without a joint subluxation. Mallet fragment angle was 55°. (B) Extension block technique was performed. (C) At postoperative 3 months, the fracture was united and the joint was congruent. Excellent result was noted according to the Crawford classification.

Figure 3 Lateral radiograph of right 5th finger. (A) Fourteen days ago, a 24-year-old male patient had an injury on his right 5th finger. Preoperative radiograph showed 50 percents of joint involvement with a joint subluxation. Mallet fragment angle was 20°. (B) Extension block technique was performed. (C) At postoperative 3 months, the fracture was united but the joint was incongruent. Fair result was noted according to the Crawford classification.
Cited by 2 articles
-
Reduction Loss after Extension Block Kirschner Wire Fixation for Treatment of Bony Mallet Finger
Byungsung Kim, Jae-Hwi Nho, Ki Jin Jung, Keonhee Yun, Eunseok Park, Sungyong Park
Arch Hand Microsurg. 2018;23(4):239-247. doi: 10.12790/ahm.2018.23.4.239.Osteoarthritis after Extension Block Technique for the Bony Mallet Finger
Sung Hoon Koh, Jung Hyun Park, Jin Soo Kim, Si Young Roh, Kyung Jin Lee, Dong Chul Lee
Arch Hand Microsurg. 2021;26(4):238-244. doi: 10.12790/ahm.21.0129.
Reference
-
1. Lester B, Jeong GK, Perry D, Spero L. A simple effective splinting technique for the mallet finger. Am J Orthop (Belle Mead NJ). 2000. 29:202–206.2. Lubahn JD. Mallet finger fractures: a comparison of open and closed technique. J Hand Surg Am. 1989. 14:394–396.
Article3. Crawford GP. The molded polythene splint for mallet finger deformities. J Hand Surg Am. 1984. 9:231–237.
Article4. Abouna JM, Brown H. The treatment of mallet finger. The results in a series of 148 consecutive cases and a review of the literature. Br J Surg. 1968. 55:653–667.
Article5. Casscells SW, Strange TB. Intramedullary-wire fixation of mallet finger. J Bone Joint Surg Am. 1969. 51:1018–1019.
Article6. Jupiter JB, Sheppard JE. Tension wire fixation of avulsion fractures in the hand. Clin Orthop Relat Res. 1987. 214:113–120.
Article7. Ishiguro T, Inoue K, Matsubayashi N, Ito Y, Hashizume N. A new method of closed reduction for mallet fractures. Cent Jpn J Orthop Trauma Surg. 1988. 31:2049–2051.8. Inoue G. Closed reduction of mallet fractures using extension-block Kirschner wire. J Orthop Trauma. 1992. 6:413–415.
Article9. Bischoff R, Buechler U, De Roche R, Jupiter J. Clinical results of tension band fixation of avulsion fractures of the hand. J Hand Surg Am. 1994. 19:1019–1026.
Article10. Damron TA, Engber WD. Surgical treatment of mallet finger fractures by tension band technique. Clin Orthop Relat Res. 1994. 300:133–140.
Article11. Ihn JC, Kim PT, Kim SY, Han S. Closed reduction of mallet fractures using extension block Kirchner wire. J Korean Orthop Assoc. 1994. 29:1593–1596.12. Ishiguro T, Itoh Y, Yabe Y, Hashizume N. Extension block with Kirschner wire for fracture dislocation of the distal interphalangeal joint. Tech Hand Up Extrem Surg. 1997. 1:95–102.
Article13. Kronlage SC, Faust D. Open reduction and screw fixation of mallet fractures. J Hand Surg Br. 2004. 29:135–138.
Article14. Darder-Prats A, Fernández-García E, Fernández-Gabarda R, Darder-García A. Treatment of mallet finger fractures by the extension-block K-wire technique. J Hand Surg Br. 1998. 23:802–805.
Article15. Tetik C, Gudemez E. Modification of the extension block Kirschner wire technique for mallet fractures. Clin Orthop Relat Res. 2002. 404:284–290.
Article16. Hofmeister EP, Mazurek MT, Shin AY, Bishop AT. Extension block pinning for large mallet fractures. J Hand Surg Am. 2003. 28:453–459.
Article17. Badia A, Riano F. A simple fixation method for unstable bony mallet finger. J Hand Surg Am. 2004. 29:1051–1055.
Article18. Kalainov DM, Hoepfner PE, Hartigan BJ, Carroll Ct 4th, Genuario J. Nonsurgical treatment of closed mallet finger fractures. J Hand Surg Am. 2005. 30:580–586.
Article19. Wehbé MA, Schneider LH. Mallet fractures. J Bone Joint Surg Am. 1984. 66:658–669.
Article20. Bendre AA, Hartigan BJ, Kalainov DM. Mallet finger. J Am Acad Orthop Surg. 2005. 13:336–344.
Article21. Stark HH, Gainor BJ, Ashworth CR, Zemel NP, Rickard TA. Operative treatment of intra-articular fractures of the dorsal aspect of the distal phalanx of digits. J Bone Joint Surg Am. 1987. 69:892–896.
Article22. Takami H, Takahashi S, Ando M. Operative treatment of mallet finger due to intra-articular fracture of the distal phalanx. Arch Orthop Trauma Surg. 2000. 120:9–13.23. Yamanaka K, Sasaki T. Treatment of mallet fractures using compression fixation pins. J Hand Surg Br. 1999. 24:358–360.
Article24. Kang HJ, Shim DJ, Choi JC, Yoon HK, Lee SY, Hahn SB. Pulp traction technique for the operative treatment of bony mallet finger. J Korean Soc Surg Hand. 2005. 10:162–168.25. Ulusoy MG, Karalezli N, Kocer U, et al. Pull-in suture technique for treatment of mallet finger. Plast Reconstr Surg. 2006. 118:696–702.26. Teoh LC, Lee JY. Mallet fractures: a novel approach to internal fixation using a hook plate. J Hand Surg Eur Vol. 2007. 32:24–30.
Article27. Rocchi L, Genitiempo M, Fanfani F. Percutaneous fixation of mallet fractures by the "umbrella handle" technique. J Hand Surg Br. 2006. 31:407–412.
Article28. Garberman SF, Diao E, Peimer CA. Mallet finger: results of early versus delayed closed treatment. J Hand Surg Am. 1994. 19:850–852.
Article29. Kang HJ, Lee WS, Hahn SB, Kang ES. Complications of bony mallet finger after operative treatement. J Korean Soc Surg Hand. 1998. 3:10–17.30. Suh JS, Lee CS, Kim YJ. Treatment of mallet finger fracture by extension block k-wire fixation. J Korean Orthop Assoc. 2008. 43:316–321.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Result of the Modified Extension Block Technique in Bony Mallet Finger
- Modified Extension Block Technique Using Conjoined Kirschner Wires for Bony Mallet Fingers
- Treatment of Mallet Finger Fracture by Extension Block K-wire Fixation
- Treatment of Bony Mallet Finger: Closed Reduction Using Extension Block K-wire
- Current concepts in traumatic mallet finger management
