Upper Cervical Subluxation and Cervicomedullary Junction Compression in Patients with Rheumatoid Arthritis
- Affiliations
-
- 1Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea. pkh2325@hanyang.ac.kr
- KMID: 2463658
- DOI: http://doi.org/10.3340/jkns.2018.0234
Abstract
OBJECTIVE
Rheumatoid arthritis (RA) is known to involve the cervical spine up to 86%. It often causes cervical instability like atlantoaxial subluxation (AAS), subaxial subluxation, and vertical subluxation (VS). In order to find the relation between RA and cord compression, we will evaluate the characteristics and risk factors of basilar invagination (BI) and cervicomedullary junction (CMJ) compression.
METHODS
From January 2007 to May 2015, 12667 patients administrated to Hanyang University Medical Center. Four thousand three hundred eighty-six patients took cervical X-ray and 250 patients took cervical computed tomography or magnetic resonance imaging. Radiologic parameters, medication records were obtained from 242 patients. Multivariate logistic regression analysis was performed with correlation of CMJ compression, basin-dental interval (BDI), basin-posterior axial line interval (BAI), pannus formation, BI, and AAS.
RESULTS
In the point of CMJ compression, atlantodental interval (ADI), posterior-atlantodental interval, BAI, AAS, and BI are relatively highly correlated. Patients with BI have 82 times strong possibility of radiologic confirmed CMJ compression, while AAS has 6-fold and pannus formation has the 3-fold possibility. Compared to the low incidence of BI, AAS and pannus formation have more proportion in CMJ compression. Furthermore, wrist joint erosion was correlated with VS and AAS.
CONCLUSION
BI has a very strong possibility of CMJ compression, while AAS and pannus formation have a high proportion in CMJ compression. Hence bilateral wrist joint erosion can be used as an indicator for the timing of screening test for cervical involvement. We suggest the early recommendation of cervical spine examination for the diagnosis of cervical involvement in order to prevent morbidity and mortality.
MeSH Terms
Figure
-

Fig. 1. Flow chart of the process for selecting eligible patients for present study. RA : rheumatoid arthritis, OPD : out patient department, HYMC : Hanyang University Medical Center, WNL : with in normal limit, Ant. : anterior, ADS : atlantodental subluxation, VS : vertical subluxation, MRI : magnetic resonance imaging, CT : computed tomography, AAS : atlantoaxial subluxation, pVD : pathologic vertical dislocation, BI : basilar invagination, SAS : subaxial subluxation.
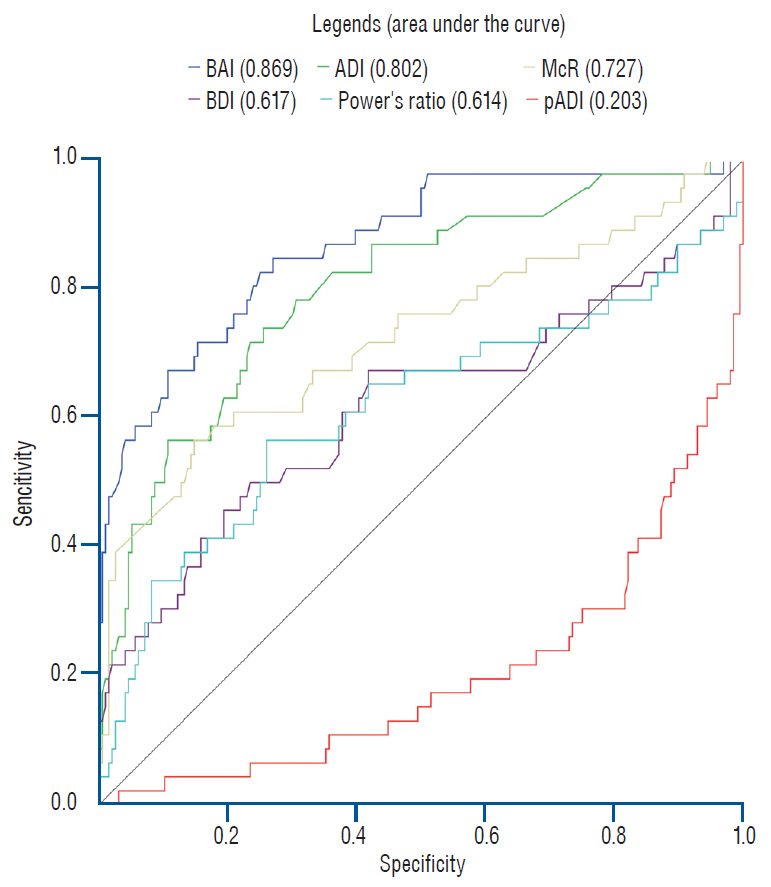
Fig. 2. ROC curve analysis was performed in radiologic morphologic parameters. Note that area under the curve of BAI is larger than that of ADI and McR, which indicates higher sensitivity and specificity. BAI : basin-posterior axial line interval, ADI : atlantodental interval, McR : McRae’s line and the tip of odontoid process of the axis, BDI : basindental interval, pADI : posterior-atlantodental interval, ROC : receiver operating characteristics.
Reference
-
References
1. Alamanos Y, Drosos AA. Epidemiology of adult rheumatoid arthritis. Autoimmun Rev. 4:130–136. 2005.
Article2. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 62:2569–2581. 2010.
Article3. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am. 75:1282–1297. 1993.
Article4. Bouchaud-Chabot A, Lioté F. Cervical spine involvement in rheumatoid arthritis. A review. Joint Bone Spine. 69:141–154. 2002.
Article5. Caird J, Bolger C. Preoperative cervical traction in cases of cranial settling with halo ring and Mayfield skull clamp. Br J Neurosurg. 19:488–489. 2005.
Article6. Casey AT, Crockard HA, Geddes JF, Stevens J. Vertical translocation: the enigma of the disappearing atlantodens interval in patients with myelopathy and rheumatoid arthritis. Part I. clinical, radiological, and neuropathological features. J Neurosurg. 87:856–862. 1997.
Article7. Collins DN, Barnes CL, FitzRandolph RL. Cervical spine instability in rheumatoid patients having total hip or knee arthroplasty. Clin Orthop Relat Res. 127–135. 1991.
Article8. Cronin CG, Lohan DG, Mhuircheartigh JN, Meehan CP, Murphy J, Roche C. CT evaluation of Chamberlain’s, McGregor’s, and McRae’s skull-base lines. Clin Radiol. 64:64–69. 2009.
Article9. Cronin CG, Lohan DG, Mhuircheartigh JN, Meehan CP, Murphy JM, Roche C. MRI evaluation and measurement of the normal odontoid peg position. Clinical radiol. 62:897–903. 2007.
Article10. Czerny C, Grampp S, Henk CB, Neuhold A, Stiskal M, Smolen J. Rheumatoid arthritis of the craniocervical region: assessment and characterization of inflammatory soft tissue proliferations with unenhanced and contrast-enhanced CT. Eur Radiol. 10:1416–1422. 2000.
Article11. Einig M, Higer HP, Meairs S, Faust-Tinnefeldt G, Kapp H. Magnetic resonance imaging of the craniocervical junction in rheumatoid arthritis: value, limitations, indications. Skeletal radiol. 19:341–346. 1990.
Article12. Gabriel SE. The epidemiology of rheumatoid arthritis. Rheum Dis Clin North Am. 27:269–281. 2001.
Article13. Halla JT, Hardin JG Jr. The spectrum of atlantoaxial facet joint involvement in rheumatoid arthritis. Arthritis Rheum. 33:325–329. 1990.
Article14. Harris JH Jr, Carson GC, Wagner LK. Radiologic diagnosis of traumatic occipitovertebral dissociation: 1. normal occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roentgenol. 162:881–886. 1994.
Article15. Harris JH Jr, Carson GC, Wagner LK, Kerr N. Radiologic diagnosis of traumatic occipitovertebral dissociation: 2. comparison of three methods of detecting occipitovertebral relationships on lateral radiographs of supine subjects. AJR Am J Roentgenol. 162:887–892. 1994.
Article16. Isdale IC, Conlon PW. Atlanto-axial subluxation. A six-year follow-up report. Ann Rheum Dis. 30:387–389. 1971.
Article17. Kauppi M, Sakaguchi M, Konttinen YT, Hämäläinen M. A new method of screening for vertical atlantoaxial dislocation. J Rheumatol. 17:167–172. 1990.18. Kauppi M, Sakaguchi M, Konttinen YT, Hämäläinen M, Hakala M. Pathogenetic mechanism and prevalence of the stable atlantoaxial subluxation in rheumatoid arthritis. J Rheumatol. 23:831–834. 1996.19. Kim SJ, Ishibashi T, Saito H, Maruoka S, Higano S, Sato A, et al. New methods for measuring atlanto-axial vertical subluxation in rheumatoid arthritis by MR imaging. Nihon Igaku Hoshasen Gakkai Zasshi. 58:94–96. 1998.20. Komusi T, Munro T, Harth M. Radiologic review: the rheumatoid cervical spine. Semin Arthritis Rheum. 14:187–195. 1985.
Article21. Kramer J, Jolesz F, Kleefield J. Rheumatoid arthritis of the cervical spine. Rheum Dis Clin North Am. 17:757–772. 1991.
Article22. Lewandrowski KU, Park PP, Baron JM, Curtin SL. Atraumatic odontoid fractures in patients with rheumatoid arthritis. Spine J. 6:529–533. 2006.
Article23. Lourie H, Stewart WA. Spontaneous atlantoaxial dislocation. A complication of rheumatoid disease. N Engl J Med. 265:677–681. 1961.24. Martel W. The occipito-atlanto-axial joints in rheumatoid arthritis and ankylosing spondylitis. Am J Roentgenol Radium Ther Nucl Med. 86:223–240. 1961.25. Mathews JA. Atlanto-axial subluxation in rheumatoid arthritis. Ann Rheum Dis. 28:260–266. 1969.
Article26. Mathews JA. Atlanto-axial subluxation in rheumatoid arthritis. A 5-year follow-up study. Ann Rheum Dis. 33:526–531. 1974.
Article27. McGreger M. The significance of certain measurements of the skull in the diagnosis of basilar impression. Br J Radiol. 21:171–181. 1948.
Article28. Mikulowski P, Wollheim FA, Rotmil P, Olsen I. Sudden death in rheumatoid arthritis with atlanto-axial dislocation. Acta Med Scand. 198:445–451. 1975.
Article29. Nguyen HV, Ludwig SC, Silber J, Gelb DE, Anderson PA, Frank L, et al. Rheumatoid arthritis of the cervical spine. Spine J. 4:329–334. 2004.
Article30. Pellicci PM, Ranawat CS, Tsairis P, Bryan WJ. A prospective study of the progression of rheumatoid arthritis of the cervical spine. J Bone Joint Surg Am. 63:342–350. 1981.
Article31. Rana NA. Natural history of atlanto-axial subluxation in rheumatoid arthritis. Spine (Phila Pa 1976). 14:1054–1056. 1989.
Article32. Ranawat CS, O’Leary P, Pellicci P, Tsairis P, Marchisello P, Dorr L. Cervical spine fusion in rheumatoid arthritis. J Bone Joint Surg Am. 61:1003–1010. 1979.
Article33. Redlund-Johnell I, Pettersson H. Radiographic measurements of the cranio-vertebral region. Designed for evaluation of abnormalities in rheumatoid arthritis. Acta Radiol Diagn (Stockh). 25:23–28. 1984.34. Redlund-Johnell I, Pettersson H. Vertical dislocation of the C1 and C2 vertebrae in rheumatoid arthritis. Acta Radiol Diagn (Stockh). 25:133–141. 1984.
Article35. Reiter MF, Boden SD. Inflammatory disorders of the cervical spine. Spine (Phila Pa 1976). 23:2755–2766. 1998.
Article36. Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 83-A:194–200. 2001.37. Sandhu FA, Pait TG, Benzel E, Henderson FC. Occipitocervical fusion for rheumatoid arthritis using the inside-outside stabilization technique. Spine (Phila Pa 1976). 28:414–419. 2003.
Article38. Santavirta S, Kankaanpää U, Sandelin J, Laasonen E, Konttinen YT, Slätis P. Evaluation of patients with rheumatoid cervical spine. Scand J Rheumatol. 16:9–16. 1987.39. Semble EL, Elster AD, Loeser RF, Laster DW, Challa VR, Pisko EJ. Magnetic resonance imaging of the craniovertebral junction in rheumatoid arthritis. J Rheumatol. 15:1367–1375. 1988.40. Sharp J, Purser DW. Spontaneous atlanto-axial dislocation in ankylosing spondylitis and rheumatoid arthritis. Ann Rheum Dis. 20:47–77. 1961.
Article41. Slätis P, Santavirta S, Sandelin J, Konttinen YT. Cranial subluxation of the odontoid process in rheumatoid arthritis. J Bone Joint Surg Am. 71:189–195. 1989.
Article42. Stach CM, Bäuerle M, Englbrecht M, Kronke G, Engelke K, Manger B, et al. Periarticular bone structure in rheumatoid arthritis patients and healthy individuals assessed by high-resolution computed tomography. Arthritis Rheum. 62:330–339. 2010.43. Taouli B, Guermazi A, Sack KE, Genant HK. Imaging of the hand and wrist in RA. Ann Rheum Dis. 61:867–869. 2002.
Article44. Weissman BN, Aliabadi P, Weinfeld MS, Thomas WH, Sosman JL. Prognostic features of atlantoaxial subluxation in rheumatoid arthritis patients. Radiology. 144:745–751. 1982.
Article45. Yonezawa T, Tsuji H, Matsui H, Hirano N. Subaxial lesions in rheumatoid arthritis. Radiographic factors suggestive of lower cervical myelopathy. Spine (Phila Pa 1976). 20:208–215. 1995.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Rheumatoid Arthritis Presenting Initially as Atlantoaxial Subluxation
- Surgical Management of Atlantoaxial Instability Due to Rheumatoid Arthritis
- Atlantoaxial Subluxation due to Psoriatic Arthritis
- Rheumatoid Atlantoaxial Subluxation: Report of a Case
- A Spontaneous Atlantoaxial Subluxation: A case repor
