Comparison of Retinal Ganglion Cell Damage in Glaucoma and Retinal Vein Occlusion by Visual Field
- Affiliations
-
- 1Department of Ophthalmology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea. lopilly@catholic.ac.kr
- KMID: 2445139
- DOI: http://doi.org/10.3341/jkos.2019.60.5.455
Abstract
- PURPOSE
We analyzed and compared retinal ganglion cell damage between patients with glaucoma and those with branched retinal vein occlusion (BRVO). We performed two types of visual field examinations.
METHODS
We retrospectively reviewed the medical records of 40 glaucoma eyes and 40 BRVO eyes. We compared the median deviation (MD), the pattern standard deviation (PSD), and sensitivity of damaged visual hemifield from frequency-doubling technology (FDT) C24-2 and standard automated perimetry (SAP) C24-2 visual field tests evaluation. We sought correlations between the MDs and retinal nerve fiber layer thickness as revealed by optical coherence tomography.
RESULTS
MDs did not differ between the groups. PSD value was higher in glaucoma patients with FDT C24-2 test (p = 0.022), but no difference between two groups with SAP C24-2 test (p = 0.144). In terms of the sensitivity of the damaged visual hemifield, glaucoma patients had larger areas of damage in the FDT C24-2 test (p < 0.01). In regression analyses, the log R2 values of both tests were higher in glaucoma patients.
CONCLUSIONS
Glaucoma patients had a greater damaged visual field area in the FDT C24-2 test than the SAP C24-2 test. The BRVO patients exhibited similar extents of damage in both tests. Thus, the subtypes and distributions of damaged retinal ganglion cells may differ between the conditions, facilitating differential diagnosis.
MeSH Terms
Figure
-
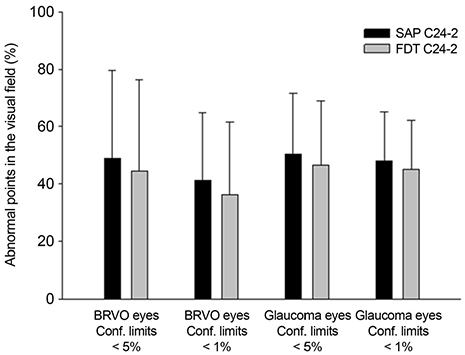
Figure 1 Percentage of abnormal points in the FDT C24-2 and SAP 24-2. It is based on confidential limits of 5% and 1% on glaucoma patients and BRVO patients. FDT = frequency doubling technique; SAP = standard automated perimetry; BRVO = branched retinal vein occlusion; Conf. limits = confidential limits.

Figure 2 Comparison as mean difference between FDT C24-2 and SAP C24-2 on glaucoma patients and BRVO patients. The percentage of the raw sensitivity points and where the confidence limit is less than 5% and 1% was calculated. FDT = frequency doubling technique; SAP = standard automated perimetry; BRVO = branched retinal vein occlusion. *The difference of raw sensitivity value from FDT C24-2 to SAP C24-2. In glaucoma patients, it was positive value but in BRVO patients, it was negative value.

Figure 3 Correlation between average RNFL thickness and median deviation categorized by diagnosis and visual field examination. (A) Glaucoma patients, FDT C24-2 (B) glaucoma patients, SAP C24-2 (C) BRVO patients, FDT C24-2 (D) BRVO patients, SAP C24-2. FDT = frequency doubling technique; SAP = standard automated perimetry; BRVO = branched retinal vein occlusion; RNFL = retinal nerve fiber layer.

Figure 4 A 41-year-old patient with NTG at superior hemifield and BRVO at inferior hemifield. (A) FDT C24-2 and SAP C24-2. On superior hemifield, the FDT C24-2 showed progressive visual defect than SAP C24-2, but on inferior hemifield two examination showed smiliar results. (B) OCT showed superior and inferior RNFL defect. (C) Disc and red-free photographs show glaucomatous cupping and localized RNFL defect. NTG = normal tension glaucoma; BRVO = branched retinal vein occlusion; FDT = frequency doubling technique; SAP = standard automated perimetry; RNFL = retinal nerve fiber layer; OCT = optical coherence tomography.
Reference
-
1. Almasieh M, Wilson AM, Morquette B, et al. The molecular basis of retinal ganglion cell death in glaucoma. Prog Retin Eye Res. 2012; 31:152–181.
Article2. Weber AJ, Chen H, Hubbard WC, Kaufman PL. Experimental glaucoma and cell size, density, and number in the primate lateral geniculate nucleus. Invest Ophthalmol Vis Sci. 2000; 41:1370–1379.3. Bayer AU, Erb C. Short wavelength automated perimetry, frequency doubling technology perimetry, and pattern electroretinography for prediction of progressive glaucomatous standard visual field defects. Ophthalmology. 2002; 109:1009–1017.
Article4. Bowd C, Zangwill LM, Berry CC, et al. Detecting early glaucoma by assessment of retinal nerve fiber layer thickness and visual function. Invest Ophthalmol Vis Sci. 2001; 42:1993–2003.5. Medeiros FA, Sample PA, Weinreb RN. Frequency doubling technology perimetry abnormalities as predictors of glaucomatous visual field loss. Am J Ophthalmol. 2004; 137:863–871.
Article6. Sample PA, Bosworth CF, Blumenthal EZ, et al. Visual function-specific perimetry for indirect comparison of different ganglion cell populations in glaucoma. Invest Ophthalmol Vis Sci. 2000; 41:1783–1790.7. Lee AJ, Wang JJ, Rochtchina E, et al. Patterns of glaucomatous visual field defects in an older population: the Blue Mountains Eye Study. Clin Exp Ophthalmol. 2003; 31:331–335.
Article8. Barbazetto IA, Schmidt-Erfurth UM. Evaluation of functional defects in branch retinal vein occlusion before and after laser treatment with scanning laser perimetry. Ophthalmology. 2000; 107:1089–1098.
Article9. Yücel YH, Zhang Q, Weinreb RN, et al. Atrophy of relay neurons in magno- and parvocellular layers in the lateral geniculate nucleus in experimental glaucoma. Invest Ophthalmol Vis Sci. 2001; 42:3216–3222.10. McKendrick AM, Sampson GP, Walland MJ, Badcock DR. Contrast sensitivity changes due to glaucoma and normal aging: low-spatial-frequency losses in both magnocellular and parvocellular pathways. Invest Ophthalmol Vis Sci. 2007; 48:2115–2122.
Article11. Yücel YH, Zhang Q, Gupta N, et al. Loss of neurons in magnocellular and parvocellular layers of the lateral geniculate nucleus in glaucoma. Arch Ophthalmol. 2000; 118:378–384.
Article12. Lamparter J, Aliyeva S, Schulze A, et al. Standard automated perimetry versus matrix frequency doubling technology perimetry in subjects with ocular hypertension and healthy control subjects. Plos One. 2013; 8:e57663.
Article13. Soliman MA, de Jong LA, Ismaeil AA, et al. Standard achromatic perimetry, short wavelength automated perimetry, and frequency doubling technology for detection of glaucoma damage. Ophthalmology. 2002; 109:444–454.
Article14. Johnson CA, Samuels SJ. Screening for glaucomatous visual field loss with frequency-doubling perimetry. Invest Ophthalmol Vis Sci. 1997; 38:413–425.15. Quigley HA. Identification of glaucoma-related visual field abnormality with the screening protocol of frequency doubling technology. Am J Ophthalmol. 1998; 125:819–829.16. Cello KE, Nelson-Quigg JM, Johnson CA. Frequency doubling technology perimetry for detection of glaucomatous visual field loss. Am J Ophthalmol. 2000; 129:314–322.
Article17. Hu R, Wang C, Racette L. Comparison of matrix frequency-doubling technology perimetry and standard automated perimetry in monitoring the development of visual field defects for glaucoma suspect eyes. PLoS One. 2017; 12:e0178079.
Article18. Patyal S, Kotwal A, Banarji A, Gurunadh VS. Frequency doubling technology and standard automated perimetry in detection of glaucoma among glaucoma suspects. Med J Armed Forces India. 2014; 70:332–337.
Article19. Alshareef RA, Barteselli G, You Q, et al. In vivo evaluation of retinal ganglion cells degeneration in eyes with branch retinal vein occlusion. Br J Ophthalmol. 2016; 100:1506–1510.
Article20. Lim HB, Kim MS, Jo YJ, Kim JY. Prediction of retinal ischemia in branch retinal vein occlusion: spectral-domain optical coherence tomography study. Invest Ophthalmol Vis Sci. 2015; 56:6622–6629.
Article21. Harwerth RS, Quigley HA. Visual field defects and retinal ganglion cell losses in patients with glaucoma. Arch Ophthalmol. 2006; 124:853–859.
Article22. Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008; 19:85–88.
Article23. Kim CS, Shin KS, Lee HJ, et al. Sectoral retinal nerve fiber layer thinning in branch retinal vein occlusion. Retina. 2014; 34:525–530.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experimental Branch Retinal Vein Occlusion in Albino Rats
- The Mechanism of Tissue Injury in the Animal Model of Experimental Retinal Vein Occlusion
- Clinical Analysis of the Hemispheric Retinal Vein Occlusion
- Apoptotic Cell Death in Experimental Retinal Vein Occlusion
- A Clinical Study on the Occlusion of the Retinal Vein
