Clinical Features of Recurred Vogt-Koyanagi-Harada Syndrome during Oral Steroids Tapering Therapy
- Affiliations
-
- 1Department of Ophthalmology, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju, Korea. cjbmed@naver.com
- KMID: 2443149
- DOI: http://doi.org/10.3341/jkos.2019.60.4.331
Abstract
- PURPOSE
To evaluate the clinical features of recurrent Vogt-Koyanagi-Harada syndrome during steroid tapering after high-dose intravenous steroid therapy.
METHODS
We retrospectively reviewed the medical records of eight patients who were diagnosed and treated for Vogt-Koyanagi-Harada syndrome from January 2010 to December 2017. Recurrence was defined as the occurrence of uveitis or serous retinal detachment during oral steroid tapering. We grouped the patients into two groups according to recurrence, and compared the best-corrected visual acuity, maximum height of subretinal fluid, central subfield thickness, choroidal thickness, average steroid tapering period and images from optical coherence tomography.
RESULTS
Seventeen patients were included and five patients (29.4%) recurred during oral steroid tapering. Patients with recurrent episodes were treated with increasing doses of oral steroid and/or oral immunosuppressant and sub-tenon injection of triamcinolone. Serous retinal detachment was completely absorbed after 24 weeks of treatment in all 17 patients, including the recurrence group and the best-corrected visual acuity was not significantly different between the two groups. The heights of the subretinal fluid and thicknesses of the central subfield before treatment were significantly higher in the recurrence group than in the non-recurrence group.
CONCLUSIONS
Serous retinal detachment can recur during oral steroid tapering after high-dose intravenous steroid treatment in patients with Vogt-Koyanagi-Harada syndrome suggesting that the height of the subretinal fluid at the fovea and central subfield thickness before treatment are factors associated with recurrence. Even in the case of recurrence, good visual prognosis can be expected after additional treatment according to the clinical situation.
MeSH Terms
Figure
-
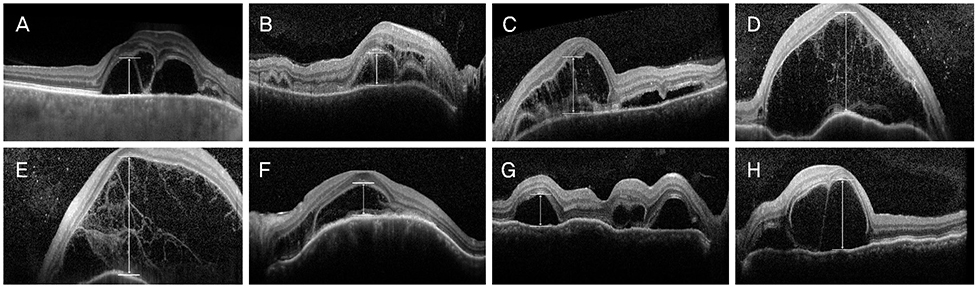
Figure 1 Optical coherence tomography images at baseline and Subretinal fluid height obtained from recurrent group. (A) Right eye of case 1. (B, C) Right and left eyes of case 2. (D, E) Right and left eyes of case 4. (F) Left eye of case 5. (G, H) Right and left eyes of case 9.
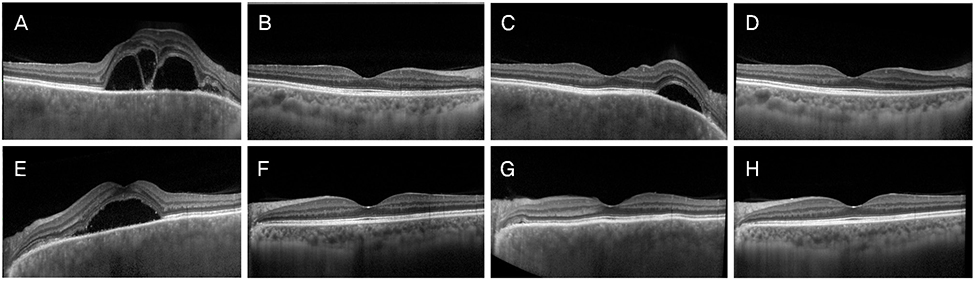
Figure 2 Optical coherence tomography (OCT) serial images obtained from case 1 of recurrent group. Left column (A–D) was OCT images of right eye, right column (E–H) was OCT images of left eye. (A, E) Serous retinal fluid (SRF) and choroidal thickening was observed at pretreatment state in both eyes. (B, F) SRF was subsided and choroidal thickness was decreased after high-dose intravenous steroid treatment. (C, G) SRF was recurred at perifoveal area during oral steroid tapering in right eye. The patient was treated with increased dose of oral steroid, oral immunosuppressant, and sub-tenon injection of triamcinolone. (D, H) SRF was completely absorbed after 24 weeks of steroid treatment.
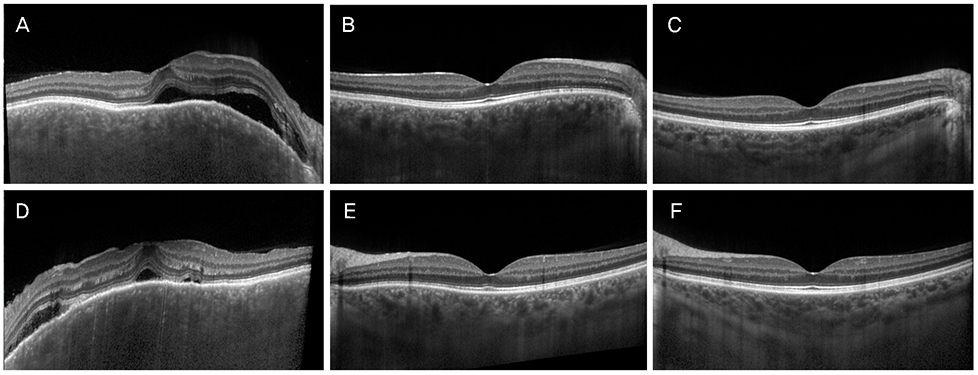
Figure 3 Optical coherence tomography (OCT) serial images obtained from case 8 of non-recurrent group. Left column (A–C) was OCT images of right eye, right column (E, F) was OCT images of left eye. (A, D) Serous retinal fluid (SRF) and choroidal thickening was observed at pretreatment state in both eyes. (B, E) SRF was subsided and choroidal thickness was decreased after high-dose intravenous steroid treatment. (C, F) OCT images after 24 weeks of high-dose intravenous steroid treatment. There was no recurrence during oral steroid tapering in both eye.
Reference
-
1. Moorthy RS, Inomata H, Rao NA. Vogt-Koyanagi-Harada syndrome. Surv Ophthalmol. 1995; 39:265–292.
Article2. Read RW, Holland GN, Rao NA, et al. Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an international committee on nomenclature. Am J Ophthalmol. 2001; 131:647–652.3. Lee JE, Park SW, Lee JK, et al. Edema of the photoreceptor layer in Vogt-Koyanagi-Harada disease observed using high-resolution optical coherence tomography. Korean J Ophthalmol. 2009; 23:74–79.
Article4. Rubsamen PE, Gass JD. Vogt-Koyanagi-Harada syndrome. Clinical course, therapy, and long-term visual outcome. Arch Ophthalmol. 1991; 109:682–687.5. Sasamoto Y, Ohno S, Matsuda H. Studies on corticosteroid therapy in Vogt-Koyanagi-Harada disease. Ophthalmologica. 1990; 201:162–167.
Article6. Bordaberry MF. Vogt-Koyanagi-Harada disease: diagnosis and treatments update. Curr Opin Ophthalmol. 2010; 21:430–435.
Article7. Kim MJ, Cho NC, Ahn M. Clinical analysis of recurrent Vogt-Koyanagi-Harada syndrome. J Korean Ophthalmol Soc. 2006; 47:227–234.8. Bykhovskaya I, Thorne JE, Kempen JH, et al. Vogt-Koyanagi-Harada disease: clinical outcomes. Am J Ophthalmol. 2005; 140:674–678.
Article9. Agarwal M, Ganesh SK, Biswas J. Triple agent immunosuppressive therapy in Vogt-Koyanagi-Harada syndrome. Ocul Immunol Inflamm. 2006; 14:333–339.
Article10. Abu El-Asrar AM, Al Tamimi M, Hemachandran S, et al. Prognostic factors for clinical outcomes in patients with Vogt-Koyanagi-Harada disease treated with high-dose corticosteroids. Acta Ophthalmol. 2013; 91:e486–e493.
Article11. Kondo Y, Fukuda K, Suzuki K, Nishida T. Chronic noninfectious uveitis associated with Vogt-Koyanagi-Harada disease treated with low-dose weekly systemic methotrexate. Jpn J Ophthalmol. 2012; 56:104–106.
Article12. Ikewaki J, Kimoto K, Choshi T, et al. Optical coherence tomographic assessment of dynamic macular changes in patients with Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2011; 31:9–13.
Article13. Nazari H, Rao NA. Resolution of subretinal fluid with systemic corticosteroid treatment in acute Vogt-Koyanagi-Harada disease. Br J Ophthalmol. 2012; 96:1410–1414.
Article14. Yamaguchi Y, Otani T, Kishi S. Tomographic features of serous retinal detachment with multilobular dye pooling in acute Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2007; 144:260–265.
Article15. Chung H, Choi DG. Clinical analysis of uveitis. Korean J Ophthalmol. 1989; 3:33–37.
Article16. Lai TY, Chan RP, Chan CK, Lam DS. Effects of the duration of initial oral corticosteroid treatment on the recurrence of inflammation in Vogt-Koyanagi-Harada disease. Eye (Lond). 2009; 23:543–548.
Article17. Abu El-Asrar AM, Hemachandran S, Al-Mezaine HS, et al. The outcomes of mycophenolate mofetil therapy combined with systemic corticosteroids in acute uveitis associated with Vogt-Koyanagi-Harada disease. Acta Ophthalmol. 2012; 90:e603–e608.
Article18. Paredes I, Ahmed M, Foster CS. Immunomodulatory therapy for Vogt-Koyanagi-Harada patients as first-line therapy. Ocul Immunol Inflamm. 2006; 14:87–90.
Article19. Sheu SJ, Kou HK, Chen JF. Prognostic factors for Vogt-Koyanagi-Harada disease. J Chin Med Assoc. 2003; 66:148–154.20. Nakayama M, Keino H, Okada AA, et al. Enhanced depth imaging optical coherence tomography of the choroid in Vogt-Koyanagi-Harada disease. Retina. 2012; 32:2061–2069.
Article21. Read RW, Rechodouni A, Butani N, et al. Complications and prognostic factors in Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2001; 131:599–606.
Article22. Sakata VM, da Silva FT, Hirata CE, et al. High rate of clinical recurrence in patients with Vogt-Koyanagi-Harada disease treated with early high-dose corticosteroids. Graefes Arch Clin Exp Ophthalmol. 2015; 253:785–790.
Article23. Iwahashi C, Okuno K, Hashida N, et al. Incidence and clinical features of recurrent Vogt-Koyanagi-Harada disease in Japanese individuals. Jpn J Ophthalmol. 2015; 59:157–163.
Article24. Sachdev N, Gupta V, Gupta A, Singh R. Posterior segment recurrences in Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2008; 28:339–345.
Article25. Nishioka Y, Sakamoto M, Kinukawa N, et al. Recurrence risk factors in patients with the Vogt-Koyanagi-Harada syndrome in Japan. Ocul Immunol Inflamm. 1995; 3:73–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vogt-Koyanagi-Harada Syndrome Associated with Psoriasis Vulgaris
- Photodynamic Therapy with Verteporfin for Subfoveal Choroidal Neovascularization in Vogt-Koyanagi-Harada Syndrome
- A Case of Vogt-Koyanagi-Harada syndrome presenting initially with recurrent vertigo
- A Case of Vogt-Koyanagi-Harada's Syndrome
- Clinical Analysis of Recurrent Vogt-Koyanagi-Harada Syndrome
