J Korean Neurosurg Soc.
2019 Mar;62(2):232-242. 10.3340/jkns.2018.0037.
Effects of Trauma Center Establishment on the Clinical Characteristics and Outcomes of Patients with Traumatic Brain Injury : A Retrospective Analysis from a Single Trauma Center in Korea
- Affiliations
-
- 1Department of Neurosurgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. kist1817@gmail.com
- 2Trauma center, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- KMID: 2441568
- DOI: http://doi.org/10.3340/jkns.2018.0037
Abstract
OBJECTIVE
To investigate the effects of trauma center establishment on the clinical characteristics and outcomes of trauma patients with traumatic brain injury (TBI).
METHODS
We enrolled 322 patients with severe trauma and TBI from January 2015 to December 2016. Clinical factors, indexes, and outcomes were compared before and after trauma center establishment (September 2015). The outcome was the Glasgow outcome scale classification at 3 months post-trauma.
RESULTS
Of the 322 patients, 120 (37.3%) and 202 (62.7%) were admitted before and after trauma center establishment, respectively. The two groups were significantly different in age (p=0.038), the trauma location within the city (p=0.010), the proportion of intensive care unit (ICU) admissions (p=0.001), and the emergency room stay time (p < ;0.001). Mortality occurred in 37 patients (11.5%). Although the preventable death rate decreased from before to after center establishment (23.1% vs. 12.5%), the difference was not significant. None of the clinical factors, indexes, or outcomes were different from before to after center establishment for patients with severe TBI (Glasgow coma scale score ≤8). However, the proportion of inter-hospital transfers increased and the time to emergency room arrival was longer in both the entire cohort and patients with severe TBI after versus before trauma center establishment.
CONCLUSION
We confirmed that for patients with severe trauma and TBI, establishing a trauma center increased the proportion of ICU admissions and decreased the emergency room stay time and preventable death rate. However, management strategies for handling the high proportion of inter-hospital transfers and long times to emergency room arrival will be necessary.
Keyword
MeSH Terms
Figure
-
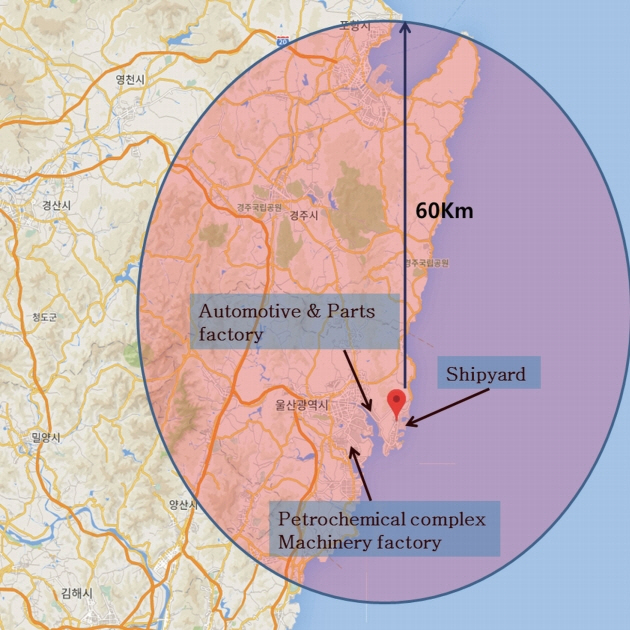
Fig. 1. Location characteristics and responsibility area of the trauma center (black spot : trauma center, black circle : responsibility area).
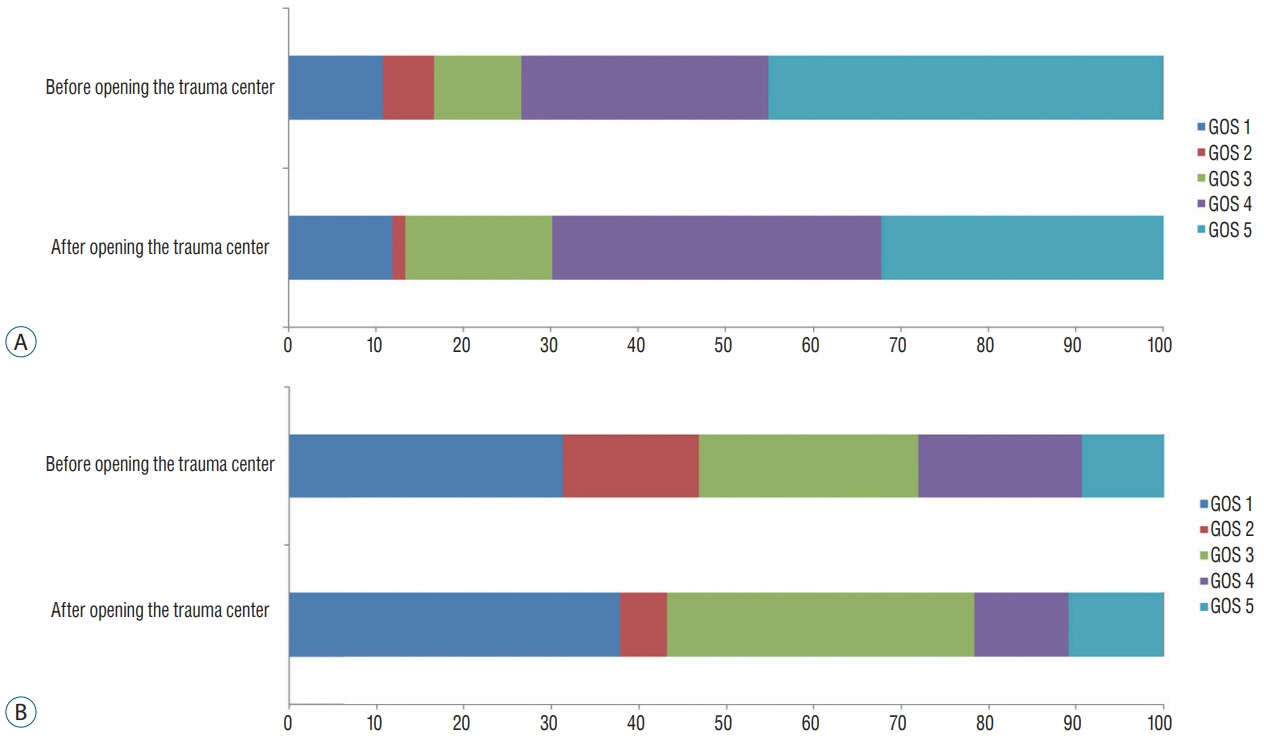
Fig. 2. GOS at 3 months after the accident for all patients (A) and patients with severe traumatic brain injury (B). GOS : Glasgow outcome scale.

Fig. 3. “Mobile Trauma Unit”, dedicated vehicle with doctors for interhospital transfers or direct treatment at the accident site.
Reference
-
References
1. Bach JA, Leskovan JJ, Scharschmidt T, Boulger C, Papadimos TJ, Russell S, et al. The right team at the right time - Multidisciplinary approach to multi-trauma patient with orthopedic injuries. Int J Crit Illn Inj Sci. 7:32–37. 2017.
Article2. Baker SP, O’Neill B, Haddon W Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 14:187–196. 1974.3. Bonatti H, Calland JF. Trauma. Emerg Med Clin North Am. 26:625–648, vii. 2008.
Article4. Champion HR, Sacco WJ, Carnazzo AJ, Copes W, Fouty WJ. Trauma score. Crit Care Med. 9:672–676. 1981.
Article5. Cherry RA, King TS, Carney DE, Bryant P, Cooney RN. Trauma team activation and the impact on mortality. J Trauma. 63:326–330. 2007.
Article6. Coronado VG, Xu L, Basavaraju SV, McGuire LC, Wald MM, Faul MD, et al. Surveillance for traumatic brain injury-related deaths--United States, 1997-2007. MMWR Surveill Summ. 60:1–32. 2011.7. El Mestoui Z, Jalalzadeh H, Giannakopoulos GF, Zuidema WP. Incidence and etiology of mortality in polytrauma patients in a Dutch level I trauma center. Eur J Emerg Med. 24:49–54. 2017.
Article8. Fröhlich M, Lefering R, Probst C, Paffrath T, Schneider MM, Maegele M, et al. Epidemiology and risk factors of multiple-organ failure after multiple trauma: an analysis of 31,154 patients from the TraumaRegister DGU. J Trauma Acute Care Surg. 76:921–927. discussion 927-928. 2014.9. Ghajar J. Traumatic brain injury. Lancet. 356:923–929. 2000.
Article10. Howard JT, Kotwal RS, Santos-Lazada AR, Martin MJ, Stockinger ZT. Reexamination of a battlefield trauma golden hour policy. J Trauma Acute Care Surg. 84:11–18. 2018.
Article11. Humphreys I, Wood RL, Phillips CJ, Macey S. The costs of traumatic brain injury: a literature review. Clinicoecon Outcomes Res. 5:281–287. 2013.
Article12. Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. 1:480–484. 1975.13. Kane G, Wheeler NC, Cook S, Englehardt R, Pavey B, Green K, et al. Impact of the Los Angeles county trauma system on the survival of seriously injured patients. J Trauma. 32:576–583. 1992.
Article14. Kim Y, Jung KY, Cho KH, Kim H, Ahn HC, Oh SH, et al. Preventable trauma deaths rates and management errors in emergency medical system in Korea. J Korean Soc Emerg Med. 17:385–394. 2006.15. Maio RF, Burney RE, Gregor MA, Baranski MG. A study of preventable trauma mortality in rural Michigan. J Trauma. 41:83–90. 1996.
Article16. Mann NC, Cahn RM, Mullins RJ, Brand DM, Jurkovich GJ. Survival among injured geriatric patients during construction of a statewide trauma system. J Trauma. 50:1111–1116. 2001.
Article17. Moon S, Lee SH, Ryoo HW, Kim JK, Ahn JY, Kim SJ, et al. Preventable trauma death rate in Daegu, South Korea. Clin Exp Emerg Med. 2:236–243. 2015.
Article18. Mullins RJ, Veum-Stone J, Helfand M, Zimmer-Gembeck M, Hedges JR, Southard PA, et al. Outcome of hospitalized injured patients after institution of a trauma system in an urban area. JAMA. 271:1919–1924. 1994.
Article19. Newgard CD, Meier EN, Bulger EM, Buick J, Sheehan K, Lin S, et al. Revisiting the “Golden Hour”: an evaluation of out-of-hospital time in shock and traumatic brain injury. Ann Emerg Med. 66:30–41, 41.e1-e3. 2015.
Article20. Palmer C. Major trauma and the injury severity score--where should we set the bar? Annu Proc Assoc Adv Automot Med. 51:13–29. 2007.21. Park JM. Outcomes of the support services for the establishment of regional level 1 trauma centers. J Korean Med Assoc. 59:923–930. 2016.
Article22. Ponsford J, Olver J, Ponsford M, Nelms R. Long-term adjustment of families following traumatic brain injury where comprehensive rehabilitation has been provided. Brain Inj. 17:453–468. 2003.
Article23. Saatman KE, Duhaime AC, Bullock R, Maas AI, Valadka A, Manley GT, et al. Classification of traumatic brain injury for targeted therapies. J Neurotrauma. 25:719–738. 2008.
Article24. Sampalis JS, Lavoie A, Boukas S, Tamim H, Nikolis A, Fréchette P, et al. Trauma center designation: initial impact on trauma-related mortality. J Trauma. 39:232–237. discussion 237-239. 1995.25. Schluter PJ. The Trauma and Injury Severity Score (TRISS) revised. Injury. 42:90–96. 2011.
Article26. Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 2:81–84. 1974.27. Teixeira PG, Inaba K, Hadjizacharia P, Brown C, Salim A, Rhee P, et al. Preventable or potentially preventable mortality at a mature trauma center. J Trauma. 63:1338–1346. discussion 1346-1347. 2007.
Article28. Ulvik A, Kvåle R, Wentzel-Larsen T, Flaatten H. Multiple organ failure after trauma affects even long-term survival and functional status. Crit Care. 11:R95. 2007.
Article29. Yoon HD. Background and progress of regional trauma center development. J Korean Med Assoc. 59:919–922. 2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Preventable Trauma Death Rates in Patients With Traumatic Brain Injury Before and After the Establishment of Regional Trauma Center: A Single Center Experience
- Changes in the clinical features and demographics of donors after brain death, before and after the establishment of a regional trauma center: 20 years of experience at a single center in Korea
- Surgical Outcomes in Patients with Simultaneous Traumatic Brain and Torso Injuries in a Single Regional Trauma Center over a 5-Year Period
- Comparison of Outcomes at Trauma Centers versus Non-Trauma Centers for Severe Traumatic Brain Injury
- Effect of trauma center operation on emergency care and clinical outcomes in patients with traumatic brain injury
