Change of Femoral Anteversion Angle in Children With Intoeing Gait Measured by Three-Dimensional Computed Tomography Reconstruction: One-Year Follow-Up Study
- Affiliations
-
- 1Department of Rehabilitation Medicine, Gyeongsang National University Hospital, Gyeongsang National University School of Medicine, Jinju, Korea. hsshin@gnu.ac.kr
- 2Department of Rehabilitation Medicine, Gyeongsang National University Changwon Hospital, Changwon, Korea.
- KMID: 2440979
- DOI: http://doi.org/10.5535/arm.2018.42.1.137
Abstract
OBJECTIVE
To evaluate femoral anteversion angle (FAA) change in children with intoeing gait depending on age, gender, and initial FAA using three-dimensional computed tomography (3D-CT).
METHODS
The 3D-CT data acquired between 2006 and 2016 were retrospectively reviewed. Children 4 to 10 years of age with symptomatic intoeing gait with follow-up interval of at least 1 year without active treatment were enrolled. Subjects were divided into three groups based on age: group 1 (≥4 and <6 years), group 2 (≥6 and <8 years), and group 3 (≥8 and <10 years). Initial and follow-up FAAs were measured using 3D-CT. Mean changes in FAAs were calculated and compared.
RESULTS
A total of 200 lower limbs of 100 children (48 males and 52 females, mean age of 6.1±1.6 years) were included. The mean follow-up period was 18.0±5.4 months. Average initial and follow-up FAA in children with intoeing gait was 31.1°±7.8° and 28.9°±8.2°, respectively. The initial FAA of group 1 was largest (33.5°±7.7°). Follow-up FAA of group 1 was significantly reduced to 28.7°±9.2° (p=0.000). FAA changes in groups 1, 2, and 3 were −6.5°±5.8°, −6.4°±5.1°, and −5.3°±4.0°, respectively. These changes of FAA were not significantly (p=0.355) different among the three age groups. However, FAA changes were higher (p=0.012) in females than those in males. In addition, FAA changes showed difference depending on initial FAA. When initial FAA was smaller than 30°, mean FAA change was −5.6°±4.9°. When initial FAA was more than 30°, mean FAA change was −6.8°±5.4° (p=0.019).
CONCLUSION
FAA initial in children with intoeing gait was the greatest in age group 1 (4-6 years). This group also showed significant FAA decrease at follow-up. FAA changes were greater when the child was a female, younger, and had greater initial FAA.
MeSH Terms
Figure
-
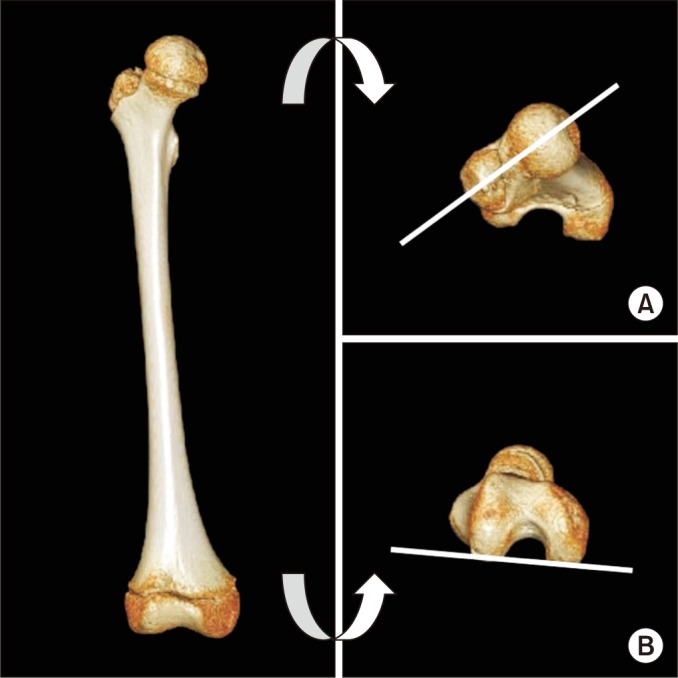
Fig. 1 Reference axes of femoral anteversion angle measurement are femoral neck axis (A) and axis between medial and lateral condyles (B).
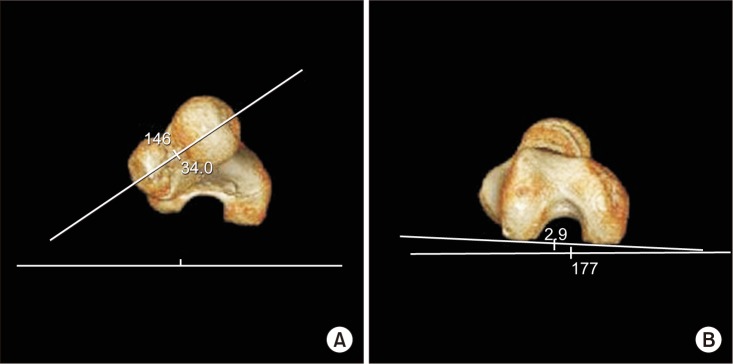
Fig. 2 Femoral anteversion angle measures the angle between long axis of femur neck (A) and transcondylar axis of the distal femur (B) from 3-dimensional computed tomography reconstruction image.
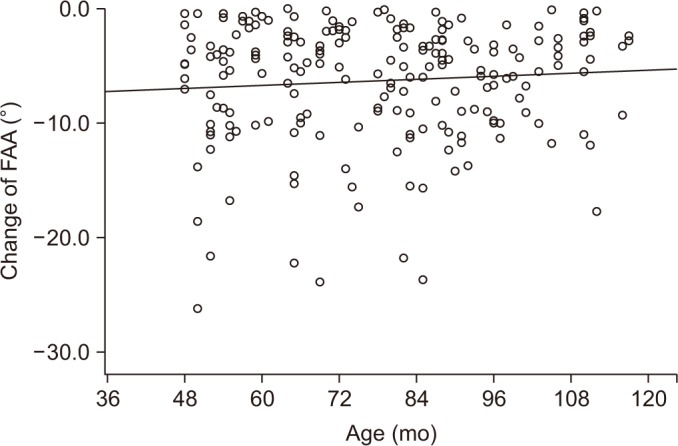
Fig. 3 Correlation between the age and change of femoral anteversion angle (FAA) at 3-dimensional computed tomography reconstruction measurement shows that more FAA change in younger children (r=0.083, p=0.243).
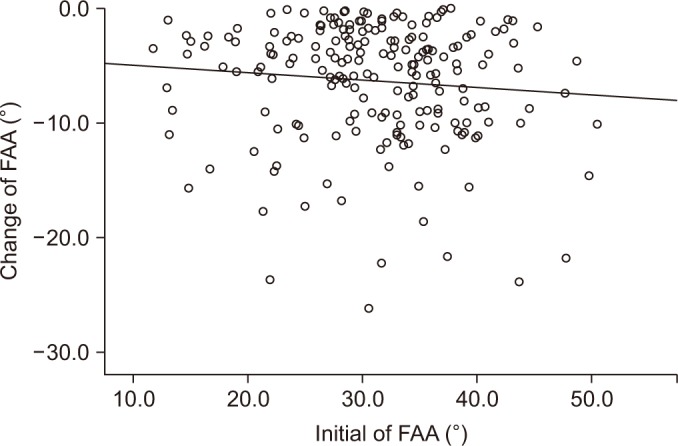
Fig. 4 Correlation between the initial femoral anteversion angle (FAA) and change of FAA at 3-dimensional computed tomography reconstruction measurement shows more FAA change with greater initial FAA (r=−0.096, p=0.018).
Cited by 1 articles
-
Change of Femoral Anteversion Angle in Children With Intoeing Gait Measured by Three-Dimensional Computed Tomography Reconstruction: 3-Year Follow-Up Study
Yeongchae Park, Hayoung Byun, Mi-Ji Kim, Heesuk Shin
Ann Rehabil Med. 2023;47(3):182-191. doi: 10.5535/arm.23043.
Reference
-
1. Valmassy RL, Lipe L, Falconer R. Pediatric treatment modalities of the lower extremity. J Am Podiatr Med Assoc. 1988; 78:69–80. PMID: 3367290.
Article2. Fabry G, Cheng LX, Molenaers G. Normal and abnormal torsional development in children. Clin Orthop Relat Res. 1994; (302):22–26.
Article3. Li YH, Leong JC. Intoeing gait in children. Hong Kong Med J. 1999; 5:360–366. PMID: 10870163.4. Fabry G, MacEwen GD, Shands AR Jr. Torsion of the femur: a follow-up study in normal and abnormal conditions. J Bone Joint Surg Am. 1973; 55:1726–1738. PMID: 4804993.5. Staheli LT, Corbett M, Wyss C, King H. Lower-extremity rotational problems in children. Normal values to guide management. J Bone Joint Surg Am. 1985; 67:39–47. PMID: 3968103.
Article6. Uden H, Kumar S. Non-surgical management of a pediatric “intoed” gait pattern: a systematic review of the current best evidence. J Multidiscip Healthc. 2012; 5:27–35. PMID: 22328828.7. Staheli LT. Torsion: treatment indications. Clin Orthop Relat Res. 1989; (247):61–66.8. Khang G, Choi K, Kim CS, Yang JS, Bae TS. A study of Korean femoral geometry. Clin Orthop Relat Res. 2003; (406):116–122.
Article9. Kim HS, Ahn KH. The hip and pelvic deformities in cerebral palsy. J Korean Acad Rehabil Med. 1994; 18:89–98.10. Park JH, Kang SY, Yoon YJ, Sung MS. A study of hip deformity in cerebral palsy. J Korean Acad Rehabil Med. 1996; 20:839–847.11. Eckhoff DG, Johnson KK. Three-dimensional computed tomography reconstruction of tibial torsion. Clin Orthop Relat Res. 1994; (302):42–46.
Article12. Gelberman RH, Cohen MS, Desai SS, Griffin PP, Salamon PB, O'Brien TM. Femoral anteversion. A clinical assessment of idiopathic intoeing gait in children. J Bone Joint Surg Br. 1987; 69:75–79. PMID: 3818738.
Article13. Davids JR, Marshall AD, Blocker ER, Frick SL, Blackhurst DW, Skewes E. Femoral anteversion in children with cerebral palsy. Assessment with two and three-dimensional computed tomography scans. J Bone Joint Surg Am. 2003; 85-A:481–488. PMID: 12637435.14. Lee S, Choi KS, Jeung IS, Lee JE, Yang SM, Lee SM. Physical examination and computed tomography in children with toe in gait. J Korean Acad Rehabil Med. 2011; 35:61–66.15. Kim HD, Lee DS, Eom MJ, Hwang JS, Han NM, Jo GY. Relationship between Physical Examinations and Two-Dimensional Computed Tomographic Findings in Children with Intoeing Gait. Ann Rehabil Med. 2011; 35:491–498. PMID: 22506164.
Article16. Rengier F, Mehndiratta A, von Tengg-Kobligk H, Zechmann CM, Unterhinninghofen R, Kauczor HU, et al. 3D printing based on imaging data: review of medical applications. Int J Comput Assist Radiol Surg. 2010; 5:335–341. PMID: 20467825.
Article17. Flohr TG, Schaller S, Stierstorfer K, Bruder H, Ohnesorge BM, Schoepf UJ. Multi-detector row CT systems and image-reconstruction techniques. Radiology. 2005; 235:756–773. PMID: 15833981.
Article18. Kim JS, Park TS, Park SB, Kim JS, Kim IY, Kim SI. Measurement of femoral neck anteversion in 3D. Part 1: 3D imaging method. Med Biol Eng Comput. 2000; 38:603–609. PMID: 11217876.
Article19. Jakob RP, Haertel M, Stussi E. Tibial torsion calculated by computerized tomography and compared to other methods of measurement. J Bone Joint Surg Br. 1980; 62-B:238–242. PMID: 7364840.20. Riccio AI, Carney CD, Hammel LC, Stanley M, Cassidy J, Davids JR. Three-dimensional computed tomography for determination of femoral anteversion in a cerebral palsy model. J Pediatr Orthop. 2015; 35:167–171. PMID: 25668788.
Article21. Byun HY, Shin H, Lee ES, Kong MS, Lee SH, Lee CH. The availability of radiological measurement of femoral anteversion angle: three-dimensional computed tomography reconstruction. Ann Rehabil Med. 2016; 40:237–243. PMID: 27152273.
Article22. Guenther KP, Tomczak R, Kessler S, Pfeiffer T, Puhl W. Measurement of femoral anteversion by magnetic resonance imaging: evaluation of a new technique in children and adolescents. Eur J Radiol. 1995; 21:47–52. PMID: 8654459.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between Femoral Anteversion and Tibial Torsion in Intoeing Gait
- Change of Femoral Anteversion Angle in Children With Intoeing Gait Measured by Three-Dimensional Computed Tomography Reconstruction: 3-Year Follow-Up Study
- Relationship between Physical Examinations and Two-Dimensional Computed Tomographic Findings in Children with Intoeing Gait
- The Availability of Radiological Measurement of Femoral Anteversion Angle: Three-Dimensional Computed Tomography Reconstruction
- Physical Examination and Computed Tomography in Children with Toe in Gait
