Aesthetic treatment of frontal sinus fractures and their complications
- Affiliations
-
- 1Department of Plastic and Reconstructive Surgery, Chonnam National University Medical School, Gwangju, Korea. pskim@chonnam.ac.kr
- KMID: 2429337
- DOI: http://doi.org/10.5124/jkma.2018.61.12.732
Abstract
- The frontal sinus is a functionally important structure. It serves as a cushioning buffer to protect the brain in cases of facial trauma. Fractures of the frontal sinus can lead to aesthetic problems by causing a visible depression in the center of the forehead. The goals of frontal sinus fracture treatment have been to protect intracranial structures and to prevent early and late complications, even with invasive methods. Recently, however, the goals have shifted to preservation of nasofrontal outflow tract function through close observation and the utilization of endoscopic procedures. Excellent cosmetic results can be achieved through minimally invasive surgery. This shift in goals took place due to the ease of diagnosis and treatment of early and late complications. Therefore, patients with a frontal sinus fracture should be followed up continuously to ensure that complications are detected promptly. Herein, the authors describe the methods and current trends of frontal sinus fracture treatment.
Keyword
MeSH Terms
Figure
-

Figure 1. Sagittal view showing a well-pneumatized frontal sinus in a 21-year-old man.
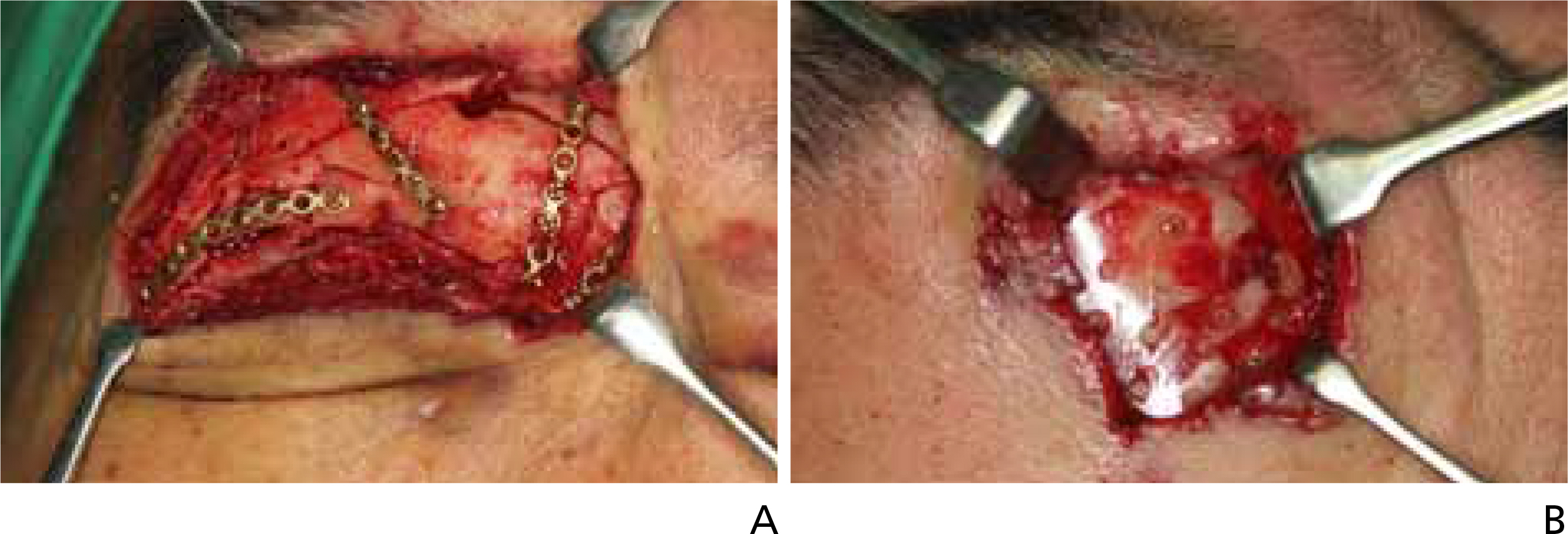
Figure 2. Materials for internal fixation. (A) Titanium plates and screws. (B) Absorbable mesh plate and screws. Informed consent was obtained from the patient.

Figure 3. A 16-year-old boy with a right frontal sinus fracture due to a sports injury. (A,B) Preoperative computed tomograms demonstrating a right anterior table frontal sinus fracture. (C,D) Postoperative computed tomograms demonstrating a well-reconstructed anterior table of the frontal sinus in the proper position.
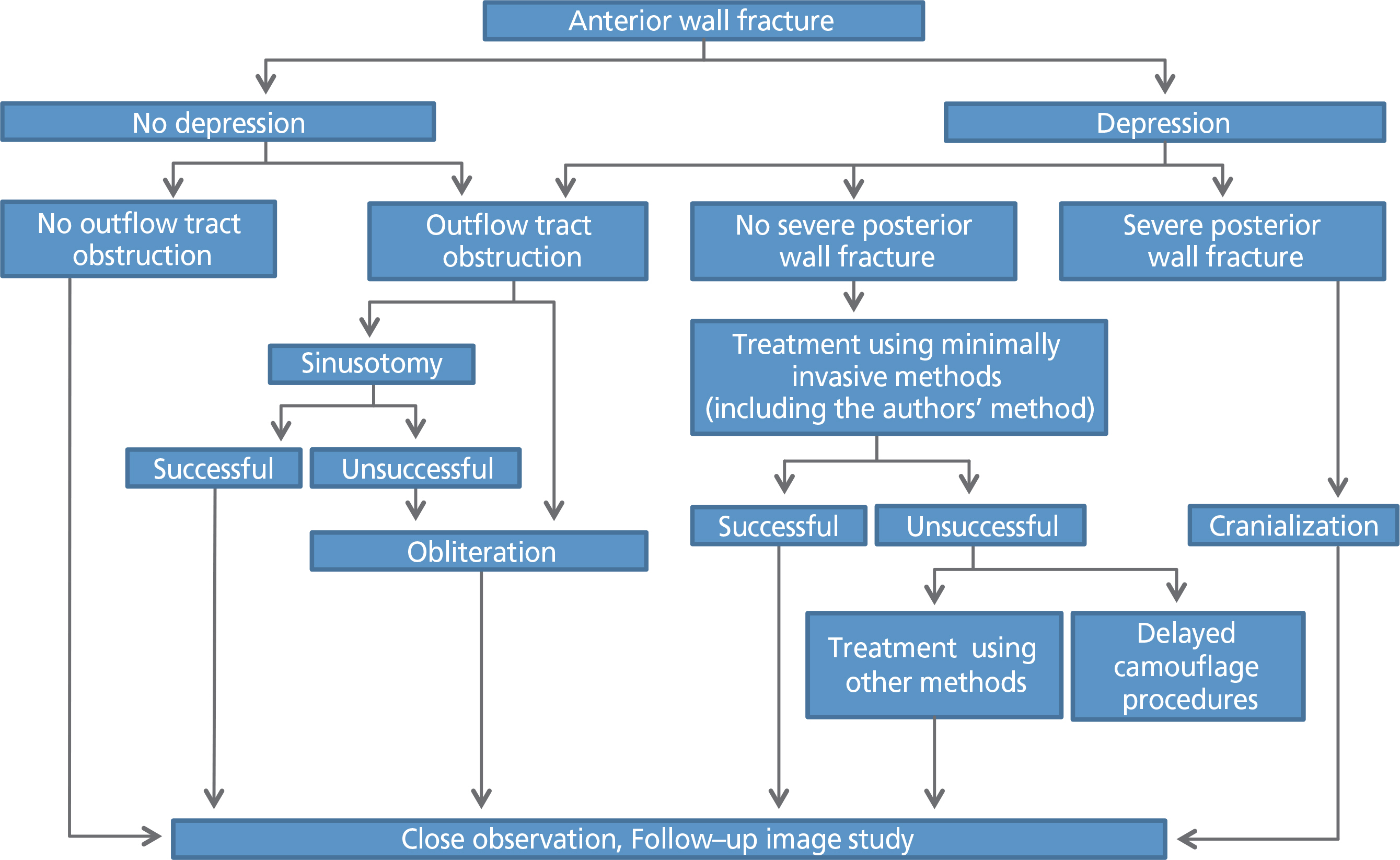
Figure 4. Algorithm for the treatment of frontal sinus fractures
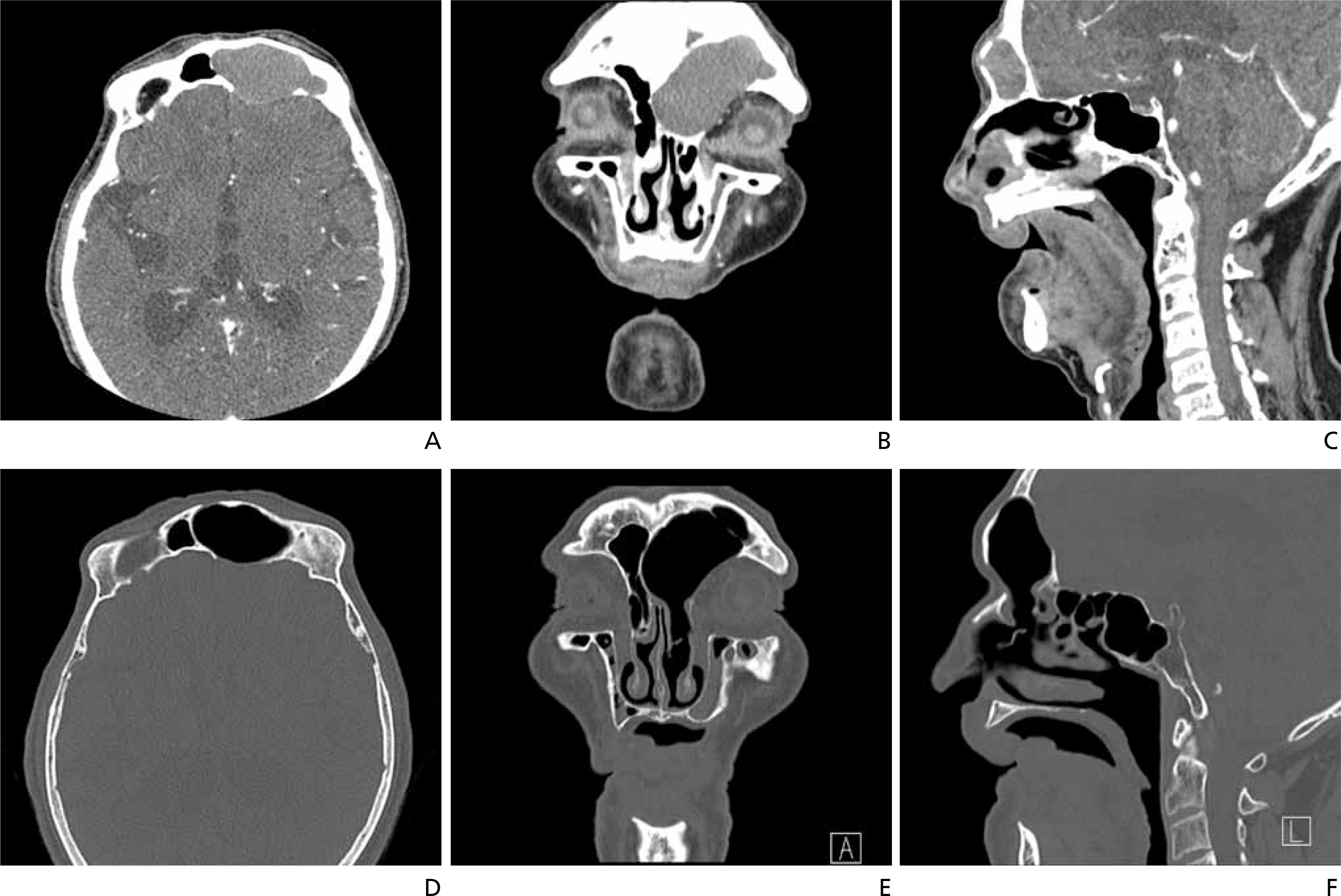
Figure 5. A 64-year-old man with a large frontal mucocele occurring 30 years after frontal sinus fracture. (A-C) Preoperative computed tomograms. (D-F) Computed tomograms after endoscopic intranasal frontal sinusotomy.
Reference
-
1. Echo A, Troy JS, Hollier LH Jr. Frontal sinus fractures. Semin Plast Surg. 2010; 24:375–382.
Article2. Schultz K, Braun TL, Truong TA. Frontal sinus fractures. Semin Plast Surg. 2017; 31:80–84.
Article3. Choi M, Li Y, Shapiro SA, Havlik RJ, Flores RL. A 10-year review of frontal sinus fractures: clinical outcomes of conservative management of posterior table fractures. Plast Reconstr Surg. 2012; 130:399–406.4. Weathers WM, Wolfswinkel EM, Hatef DA, Lee EI, Brown RH, Hollier LH Jr. Frontal sinus fractures: a conservative shift. Craniomaxillofac Trauma Reconstr. 2013; 6:155–160.
Article5. MacIsaac ZM, Naran S, Losee JE. Pediatric frontal sinus fracture conservative care: complete remodeling with growth and development. J Craniofac Surg. 2013; 24:1838–1840.6. Manson PN. Facial fractures. Mathes SJ, Hentz VR, editors. editors.Plastic surgery. 2nd ed.Philadelphia: Saunders Elsevier;2006. p. 338–344.7. Manolidis S, Hollier LH Jr. Management of frontal sinus fractures. Plast Reconstr Surg. 2007; 120(7 Suppl 2):32S–48S.
Article8. Kim TH, Kang SJ, Sun H. Delayed degradation according to the location of fixation with using an absorbable plate. Arch Craniofac Surg. 2018; 19:114–119.
Article9. Jeon HB, Kang DH, Gu JH, Oh SA. Delayed foreign body reaction caused by bioabsorbable plates used for maxillofacial fractures. Arch Plast Surg. 2016; 43:40–45.
Article10. Hwang K, Song YB. Closed reduction of fractured anterior wall of the frontal bone. J Craniofac Surg. 2005; 16:120–122.
Article11. Kim NH, Kang SJ. A simple aesthetic approach for correction of frontal sinus fracture. J Craniofac Surg. 2014; 25:544–546.
Article12. Yoo A, Eun SC, Baek RM. Transcutaneous reduction of frontal sinus fracture using bony tapper device. J Craniofac Surg. 2012; 23:1835–1837.
Article13. Hahn HM, Lee YJ, Park MC, Lee IJ, Kim SM, Park DH. Reduction of closed frontal sinus fractures through suprabrow approach. Arch Craniofac Surg. 2017; 18:230–237.
Article14. Lee Y, Choi HG, Shin DH, Uhm KI, Kim SH, Kim CK, Jo DI. Subbrow approach as a minimally invasive reduction technique in the management of frontal sinus fractures. Arch Plast Surg. 2014; 41:679–685.
Article15. Steiger JD, Chiu AG, Francis DO, Palmer JN. Endoscopic-assisted reduction of anterior table frontal sinus fractures. Laryngoscope. 2006; 116:1936–1939.
Article16. Becker SS, Bomeli SR, Gross CW, Han JK. Limits of endoscopic visualization and instrumentation in the frontal sinus. Otolaryngol Head Neck Surg. 2006; 135:917–921.
Article17. Lappert PW, Lee JW. Treatment of an isolated outer table frontal sinus fracture using endoscopic reduction and fixation. Plast Reconstr Surg. 1998; 102:1642–1645.
Article18. Kim KS, Kim ES, Hwang JH, Lee SY. Transcutaneous transfrontal approach through a small peri-eyebrow incision for the reduction of closed anterior table frontal sinus fractures. J Plast Reconstr Aesthet Surg. 2010; 63:763–768.
Article19. Kim J, Yang HJ, Kim JH, Kim SJ. Reduction of the isolated anterior wall of the maxillary sinus fracture with double urinary balloon catheters and fibrin glue. Arch Craniofac Surg. 2017; 18:238–242.
Article20. Kim KK, Mueller R, Huang F, Strong EB. Endoscopic repair of anterior table: frontal sinus fractures with a Medpor implant. Otolaryngol Head Neck Surg. 2007; 136:568–572.
Article21. Rodriguez ED, Stanwix MG, Nam AJ, St Hilaire H, Simmons OP, Christy MR, Grant MP, Manson PN. Twenty-six-year experience treating frontal sinus fractures: a novel algorithm based on anatomical fracture pattern and failure of conventional techniques. Plast Reconstr Surg. 2008; 122:1850–1866.
Article22. Rohrich RJ, Hollier LH. Management of frontal sinus fractures: changing concepts. Clin Plast Surg. 1992; 19:219–232.23. Kim YH, Kim BK. Approach to frontal sinus outflow tract injury. Arch Craniofac Surg. 2017; 18:1–4.
Article24. Guy WM, Brissett AE. Contemporary management of traumatic fractures of the frontal sinus. Otolaryngol Clin North Am. 2013; 46:733–748.
Article25. Bellamy JL, Molendijk J, Reddy SK, Flores JM, Mundinger GS, Manson PN, Rodriguez ED, Dorafshar AH. Severe infectious complications following frontal sinus fracture: the impact of operative delay and perioperative antibiotic use. Plast Reconstr Surg. 2013; 132:154–162.26. Brodie HA. Prophylactic antibiotics for posttraumatic cerebrospinal fluid fistulae: a metaanalysis. Arch Otolaryngol Head Neck Surg. 1997; 123:749–752.
Article27. Castro B, Walcott BP, Redjal N, Coumans JV, Nahed BV. Cerebrospinal fluid fistula prevention and treatment following frontal sinus fractures: a review of initial management and outcomes. Neurosurg Focus. 2012; 32:E1.
Article28. Seo BF, Kang KJ, Jung SN, Byeon JH. Skeletal cavernous hemangiomas of the frontal bone with orbital roof and rim involvement. Arch Craniofac Surg. 2018; 19:214–217.
Article29. Kim J, Chang H, Jeong EC. Sinonasal intestinal-type adenocarcinoma in the frontal sinus. Arch Craniofac Surg. 2018; 19:210–213.
Article30. Pyo SB, Song JK, Ju HS, Lim SY. Reconstruction of large orbital floor defect caused by maxillary sinus mucocele. Arch Craniofac Surg. 2017; 18:197–201.
Article31. Kim JY, Jung BK, Kim YS, Roh TS, Yun IS. Forehead reconstruction with a custom-made three-dimensional titanium implant in a Parry-Romberg syndrome patient. Arch Craniofac Surg. 2018; 19:135–138.
Article32. Chen TM, Wang HJ, Chen SL, Lin FH. Reconstruction of posttraumatic frontal-bone depression using hydroxyapatite cement. Ann Plast Surg. 2004; 52:303–308.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Review of Subbrow Approach in the Management of Non-Complicated Anterior Table Frontal Sinus Fracture
- Approach to Frontal Sinus Outflow Tract Injury
- A Simplified Treatment Algorithm of Frontal Sinus Fractures: A Paradigm Shift?
- Secondary Reconstruction of Frontal Sinus Fracture
- Management of the Frontal Sinus Fracture
