Predictive Values of Magnetic Resonance Imaging Features for Tracheostomy in Traumatic Cervical Spinal Cord Injury
- Affiliations
-
- 1Department of Neurosurgery, Gil Medical Center, Gachon University College of Medicine, Incheon, Korea. samddal@gilhospital.com
- KMID: 2420066
- DOI: http://doi.org/10.3340/jkns.2017.0222
Abstract
OBJECTIVE
To evaluate the magnetic resonance (MR) imaging features that have a statistically significant association with the need for a tracheostomy in patients with cervical spinal cord injury (SCI) during the acute stage of injury.
METHODS
This study retrospectively reviewed the clinical data of 130 patients with cervical SCI. We analyzed the factors believed to increase the risk of requiring a tracheostomy, including the severity of SCI, the level of injury as determined by radiological assessment, three quantitative MR imaging parameters, and eleven qualitative MR imaging parameters.
RESULTS
Significant differences between the non-tracheostomy and tracheostomy groups were determined by the following five factors on multivariate analysis : complete SCI (p=0.007), the radiological level of C5 and above (p=0.038), maximum canal compromise (MCC) (p=0.010), lesion length (p=0.022), and osteophyte formation (p=0.015). For the MCC, the cut-off value was 46%, and the risk of requiring a tracheostomy was three times higher at an interval between 50-60% and ten times higher between 60-70%. For lesion length, the cut-off value was 20 mm, and the risk of requiring a tracheostomy was two times higher at an interval between 20-30 mm and fourteen times higher between 40-50 mm.
CONCLUSION
The American Spinal Injury Association grade A, a radiological injury level of C5 and above, an MCC ≥50%, a lesion length ≥20 mm, and osteophyte formation at the level of injury were considered to be predictive values for requiring tracheostomy intervention in patients with cervical SCI.
Keyword
MeSH Terms
Figure
-
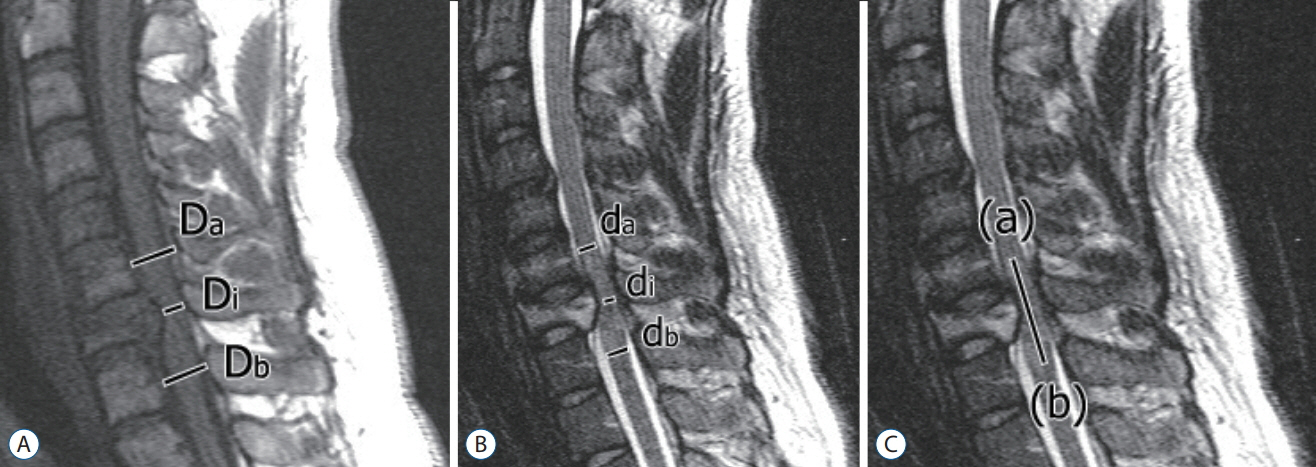
Fig. 1. Measurement of maximum canal compromise, maximum spinal cord compression, and lesion length. Midsagittal (A) T1-weighted and (B and C) T2-weighted MR images obtained in a 44-year-old man with acute traumatic cervical spinal cord injury. A : Maximum canal compromise=1-DiDa+Db/2 ×100%. B : Maximum spinal cord compression=1-DiDa+Db/2 ×100%. C : Lesion length is measured by the distance from the most cephalic extent (a) to the most caudal extent (b) of the injury. Di: the anteroposterior canal diameter at the level of maximum injury, Da: the anteroposterior canal diameter at the nearest normal level above the level of injury, Db: the anteroposterior canal diameter at the nearest normal level below the level of injury, di: the anteroposterior cord diameter at the level of maximum injury, da: the anteroposterior cord diameter at the nearest level above the level of injury, db: the anteroposterior cord diameter at the nearest normal level below the level of injury.
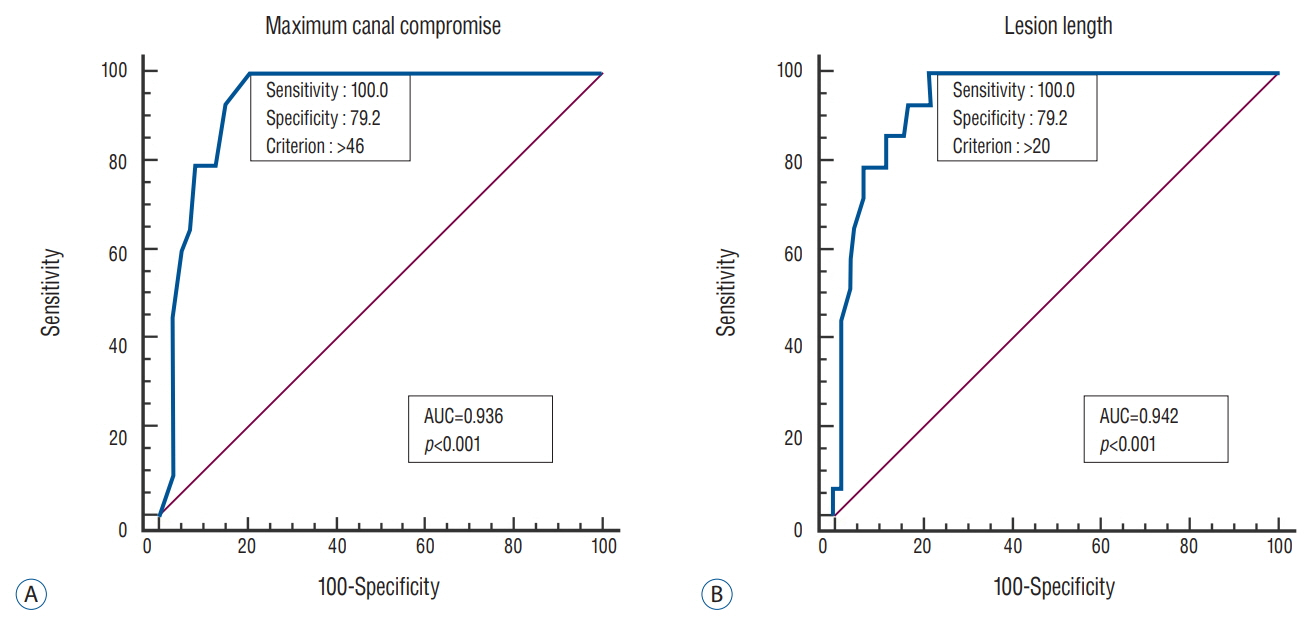
Fig. 2. Receiver operating characteristic curve. A : Maximum canal compromise. B : Lesion length. AUC : area under the receiver operating characteristic curve.
Cited by 1 articles
-
A Prognostic Factor for Prolonged Mechanical Ventilator-Dependent Respiratory Failure after Cervical Spinal Cord Injury : Maximal Canal Compromise on Magnetic Resonance Imaging
Subum Lee, Sung Woo Roh, Sang Ryong Jeon, Jin Hoon Park, Kyoung-Tae Kim, Young-Seok Lee, Dae-Chul Cho
J Korean Neurosurg Soc. 2021;64(5):791-798. doi: 10.3340/jkns.2020.0346.
Reference
-
References
1. Ball PA. Critical care of spinal cord injury. Spine (Phila Pa 1976). 26:S27–S30. 2001.
Article2. Berney S, Bragge P, Granger C, Opdam H, Denehy L. The acute respiratory management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review. Spinal Cord. 49:17–29. 2011.
Article3. Branco BC, Plurad D, Green DJ, Inaba K, Lam L, Cestero R, et al. Incidence and clinical predictors for tracheostomy after cervical spinal cord injury: a national trauma databank review. J Trauma. 70:111–115. 2011.
Article4. Brook AD, Sherman G, Malen J, Kollef MH. Early versus late tracheostomy in patients who require prolonged mechanical ventilation. Am J Crit Care. 9:352–359. 2000.
Article5. Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. 51:853–868. discussion 869-870. 2006.6. Claxton AR, Wong DT, Chung F, Fehlings MG. Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Can J Anaesth. 45:144–149. 1998.
Article7. Como JJ, Sutton ER, McCunn M, Dutton RP, Johnson SB, Aarabi B, et al. Characterizing the need for mechanical ventilation following cervical spinal cord injury with neurologic deficit. J Trauma. 59:912–916. discussion 916. 2005.
Article8. Fehlings MG, Furlan JC, Massicotte EM, Arnold P, Aarabi B, Harrop J, et al. Interobserver and intraobserver reliability of maximum canal compromise and spinal cord compression for evaluation of acute traumatic cervical spinal cord injury. Spine (Phila Pa 1976). 31:1719–1725. 2006.
Article9. Fehlings MG, Rao SC, Tator CH, Skaf G, Arnold P, Benzel E, et al. The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal cord injury. Part II: results of a multicenter study. Spine (Phila Pa 1976). 24:605–613. 1999.
Article10. Fletcher DJ, Taddonio RF, Byrne DW, Wexler LM, Cayten CG, Nealon SM, et al. Incidence of acute care complications in vertebral column fracture patients with and without spinal cord injury. Spine (Phila Pa 1976). 20:1136–1146. 1995.
Article11. Galeiras Vázquez R, Rascado Sedes P, Mourelo Fariña M, Montoto Marqués A, Ferreiro Velasco ME. Respiratory management in the patient with spinal cord injury. Biomed Res Int. 2013:168757. 2013.
Article12. Hagen EM, Lie SA, Rekand T, Gilhus NE, Gronning M. Mortality after traumatic spinal cord injury: 50 years of follow-up. J Neurol Neurosurg Psychiatry. 81:368–373. 2010.
Article13. Harrop JS, Sharan AD, Scheid EH Jr, Vaccaro AR, Przybylski GJ. Tracheostomy placement in patients with complete cervical spinal cord injuries: American Spinal Injury Association Grade A. J Neurosurg. 100(1 Suppl Spine):20–23. 2004.
Article14. Kang JD, Figgie MP, Bohlman HH. Sagittal measurements of the cervical spine in subaxial fractures and dislocations. An analysis of two hundred and eighty-eight patients with and without neurological deficits. J Bone Joint Surg Am. 76:1617–1628. 1994.
Article15. Kelly BJ, Luce JM. The diagnosis and management of neuromuscular diseases causing respiratory failure. Chest. 99:1485–1494. 1991.
Article16. Kluger Y, Paul DB, Lucke J, Cox P, Colella JJ, Townsend RN, et al. Early tracheostomy in trauma patients. Eur J Emerg Med. 3:95–101. 1996.
Article17. Mahmood NS, Kadavigere R, Avinash KR, Rao VR. Magnetic resonance imaging in acute cervical spinal cord injury: a correlative study on spinal cord changes and 1 month motor recovery. Spinal Cord. 46:791–797. 2008.
Article18. McMichan JC, Michel L, Westbrook PR. Pulmonary dysfunction following traumatic quadriplegia. Recognition, prevention, and treatment. JAMA. 243:528–531. 1980.
Article19. Miyanji F, Furlan JC, Aarabi B, Arnold PM, Fehlings MG. Acute cervical traumatic spinal cord injury: MR imaging findings correlated with neurologic outcome--prospective study with 100 consecutive patients. Radiology. 243:820–827. 2007.
Article20. Parashari UC, Khanduri S, Bhadury S, Kohli N, Parihar A, Singh R, et al. Diagnostic and prognostic role of MRI in spinal trauma, its comparison and correlation with clinical profile and neurological outcome, according to ASIA impairment scale. J Craniovertebr Junction Spine. 2:17–26. 2011.
Article21. Ramón S, Domínguez R, Ramírez L, Paraira M, Olona M, et al. Clinical and magnetic resonance imaging correlation in acute spinal cord injury. Spinal Cord. 35:664–673. 1997.
Article22. Romero J, Vari A, Gambarrutta C, Oliviero A. Tracheostomy timing in traumatic spinal cord injury. Eur Spine J. 18:1452–1457. 2009.
Article23. Schneider RC, Cherry G, Pantek H. The syndrome of acute central cervical spinal cord injury; with special reference to the mechanisms involved in hyperextension injuries of cervical spine. J Neurosurg. 11:546–577. 1954.24. Stein DM, Menaker J, McQuillan K, Handley C, Aarabi B, Scalea TM. Risk factors for organ dysfunction and failure in patients with acute traumatic cervical spinal cord injury. Neurocrit Care. 13:29–39. 2010.
Article25. Velmahos GC, Toutouzas K, Chan L, Tillou A, Rhee P, Murray J, et al. Intubation after cervical spinal cord injury: to be done selectively or routinely? Am Surg. 69:891–894. 2003.26. Wicks AB, Menter RR. Long-term outlook in quadriplegic patients with initial ventilator dependency. Chest. 90:406–410. 1986.
Article27. Yugué I, Okada S, Ueta T, Maeda T, Mori E, Kawano O, et al. Analysis of the risk factors for tracheostomy in traumatic cervical spinal cord injury. Spine (Phila Pa 1976). 37:E1633–E1638. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Neurologic Recovery According to Early Magnetic Resonance Imaging Findings in Traumatic Cervical Spinal Cord Injuries
- Solitary Osteochondroma of the Atlas with Cervical Cord Compresion: Case Report
- The Need for Early Tracheostomy in Patients with Traumatic Cervical Cord Injury
- Magnetic Resonance Imaging of Traumatic Cervical Injury
- Morphological Analysis of the Cervical Spinal Cord, Dural Tube, and Spinal Canal by Magnetic Resonance Imaging in Normal Korean Adults
