Yonsei Med J.
2005 Jun;46(3):379-387. 10.3349/ymj.2005.46.3.379.
Neurologic Recovery According to Early Magnetic Resonance Imaging Findings in Traumatic Cervical Spinal Cord Injuries
- Affiliations
-
- 1Department and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea. kimdy@yumc.yonsei.ac.kr
- KMID: 1734073
- DOI: http://doi.org/10.3349/ymj.2005.46.3.379
Abstract
- The aim of this study was to determine the usefulness of early magnetic resonance imaging findings in predicting neurologic recovery at or below the injured level in traumatic cervical spinal cord injuries. Thirty patients with traumatic cervical spinal cord injuries were included. All of the patients received a magnetic resonance imaging and a neurologic examination in the emergency room, within 7 days of injury and at 6 months following the injury. To quantify neurologic recovery below the injured level, we modified clinical scales, particularly the motor ratio and the sensory ratio. We used the neurologic level to quantify recovery around the injured level. We assessed neurologic recovery according to MRI patterns and lesion extents. The pure hemorrhagic MRI pattern was not observed. In edematous and mixed types, the improvement of neurologic levels was not significantly different. The motor ratio and sensory ratio improved significantly more in edematous type patients than in mixed type patients. Based on MRI lesion extent, the improvement of neurologic levels was not significantly different, and motor ratio and sensory ratio improved significantly more in those with one or two segments involved than in those with more than two segments involved. In conclusion, early MRI pattern and lesion extent after traumatic cervical spinal cord injury may provide important information to help predict neurologic recovery, especially below the injured level.
MeSH Terms
Figure
-

Fig. 1 Comparison of recovery rate of motor ratio and sensory ratio between edematous type and mixed type. The recovery rate of motor ratio and sensory ratio was significantly higher in the edematous type than in the mixed type (p < 0.05).
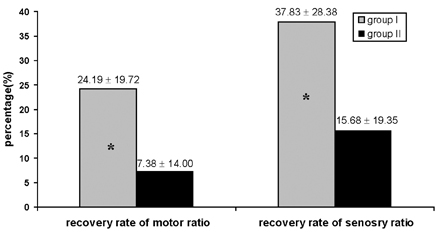
Fig. 2 Comparison of recovery rate of motor ratio and sensory ratio between groups. We classified as group I, when the alteration of intensity lies at one or two segments, and more than two segments as group II according to extent of lesion. The recovery rate of motor and sensory ratio was significantly higher in group I than in group II (p < 0.05).
Reference
-
1. Go BK, DeVivo MJ, Richards JS. Stover SI, DeLisa JA, Whiteneck GG, editors. The epidemiology of spinal cord injury. Spinal cord Injury: clinical outcomes from the model systems. 1995. 1st ed. Gaithersberg: Aspen Publishers;21–51.2. Kirshblum SC, O'Connor KC. Predicting neurologic recovery in traumatic cervical spinal cord injury. Arch Phys Med Rehabil. 1998. 79:1456–1466.3. Flanders AE, Spettell CM, Tartaglino LM, Friedman DP, Herbison GJ. Forecasting motor recovery after cervical spinal cord injury: value of MR imaging. Radiology. 1996. 201:649–655.4. York DH, Watts C, Raffensberger M, Spagnolia T, Joyce C. Utilization of somatosensory evoked cortical potentials in spinal cord injury. Prognostic limitations. Spine. 1983. 8:832–839.5. Armin C. Significance of electrophysiological recording in predicting functional recovery of patients with spinal cord injury. Neurorehabil. 1998. 10:191–203.6. Merton PA, Morton HB. Stimulation of the cerebral cortex in the intact human subject. Nature. 1980. 285:227.7. Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet. 1985. 1:1106–1107.8. Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G, Cracco RQ, et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord and roots: basic principles and procedures for routine clinical application. Report of an IFCN committee. Electroencephalogr Clin Neurophysiol. 1994. 91:79–92.9. Post MJ, Green BA. The use of computed tomography in spinal trauma. Radiol Clin North Am. 1983. 21:327–375.10. Brant-Zawadzki M, Miller EM, Federle MP. CT in the evaluation of spine trauma. Am J Roentgenol. 1981. 136:369–375.11. Virapongse C, Kier EL. Metrizamide myelography in cervical spine trauma: a modified technique using lateral fluoroscopy. Radiology. 1982. 144:636–637.12. Maynard FM Jr, Bracken MB, Creasey G, Ditunno JF Jr., Donovan WH, Ducker TB, et al. International standards for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Spinal Cord. 1997. 35:266–274.13. Blaustein DM, Zafonte R, Thomas D, Herbison GJ, Ditunno JF. Predicting recovery of motor complete quadriplegic patients. 24 hour v 72 hour motor index scores. Am J Phys Med Rehabil. 1993. 72:306–311.14. Brown PJ, Marino RJ, Herbison GJ, Ditunno JF Jr. The 72-hour examination as a predictor of recovery in motor complete quadriplegia. Arch Phys Med Rehabil. 1991. 72:546–548.15. Flanders AE, Schaefer DM, Doan HT, Mishkin MM, Gonzalez CF, Northrup BE. Acute cervical spine trauma: correlation of MR imaging findings with degree of neurologic deficit. Radiology. 1990. 177:25–33.16. Kalfas I, Wilberger J, Goldberg A, Prostko ER. Magnetic resonance imaging in acute spinal cord trauma. Neurosurgery. 1988. 23:295–299.17. Kulkarni MV, McArdle CB, Kopanicky D, Miner M, Cotler HB, Lee KF, et al. Acute spinal cord injury: MR imaging at 1.5 T. Radiology. 1987. 164:837–843.18. Perovitch M, Wang H, Perl S. The evolution of neuroimaging of spinal cord injury patients over the last decade. Paraplegia. 1992. 30:39–42.19. Schaefer DM, Flanders A, Northrup BE, Doan HT, Osterholm JL. Magnetic resonance imaging of acute cervical spine trauma. Correlation with severity of neurologic injury. Spine. 1989. 14:1090–1095.20. Silberstein M, Hennessy O. Implications of focal spinal cord lesions following trauma: evaluation with magnetic resonance imaging. Paraplegia. 1993. 31:160–167.21. Taneichi H, Abumi K, Kaneda K, Terae S. Monitoring the evolution of intramedullary lesions in cervical spinal cord injury. Qualitative and quantitative analysis with sequential MR imaging. Paraplegia. 1994. 32:9–18.22. Bondurant FJ, Cotler HB, Kulkarni MV, McArdle CB, Harris JH Jr. Acute spinal cord injury. A study using physical examination and magnetic resonance imaging. Spine. 1990. 15:161–168.23. Hayashi K, Yone K, Ito H, Yanase M, Sakou T. MRI findings in patients with a cervical spinal cord injury who do not show radiographic evidence of a fracture or dislocation. Paraplegia. 1995. 33:212–215.24. Ishida Y, Tominaga T. Predictors of neurologic recovery in acute central cervical cord injury with only upper extremity impairment. Spine. 2002. 27:1652–1658.25. Kulkarni MV, Bondurant FJ, Rose SL, Narayana PA. 1.5 tesla magnetic resonance imaging of acute spinal trauma. Radiographics. 1988. 8:1059–1082.26. Marciello MA, Flanders AE, Herbison GJ, Schaefer DM, Friedman DP, Lane JI. Magnetic resonance imaging related to neurologic outcome in cervical spinal cord injury. Arch Phys Med Rehabil. 1993. 74:940–946.27. Mascalchi M, Dal Pozzo G, Dini C, Zampa V, D'Andrea M, Mizzau M, et al. Acute spinal trauma: prognostic value of MRI appearances at 0.5 T. Clin Radiol. 1993. 48:100–108.28. Ramon S, Dominguez R, Ramirez L, Paraira M, Olona M, Castello T, et al. Clinical and magnetic resonance imaging correlation in acute spinal cord injury. Spinal Cord. 1997. 35:664–673.29. Schaefer DM, Flanders AE, Osterholm JL, Northrup BE. Prognostic significance of magnetic resonance imaging in the acute phase of cervical spine injury. J Neurosurg. 1992. 76:218–223.30. Selden NR, Quint DJ, Patel N, d'Arcy HS, Papadopoulos SM. Emergency magnetic resonance imaging of cervical spinal cord injuries: clinical correlation and prognosis. Neurosurgery. 1999. 44:785–792.31. Sett P, Crockard HA. The value of magnetic resonance imaging (MRI) in the follow-up management of spinal injury. Paraplegia. 1991. 29:396–410.32. Tator CH. Biology of neurological recovery and functional restoration after spinal cord injury. Neurosurgery. 1998. 42:696–707.33. Lucas JT, Ducker TB. Motor classification of spinal cord injuries with mobility, morbidity and recovery indices. Am Surg. 1979. 45:151–158.34. Ohta K, Fujimura Y, Nakamura M, Watanabe M, Yato Y. Experimental study on MRI evaluation of the course of cervical spinal cord injury. Spinal Cord. 1999. 37:580–584.35. Tator CH. Update on the pathophysiology and pathology of acute spinal cord injury. Brain Pathol. 1995. 5:407–413.36. Wasenko JJ, Hochhauser L, Holsapple JW, Poe LB, Albanese SA, Cacayorin ED. MR of post traumatic spinal cord lesions. Unexpected improvement of hemorrhagic lesions. Clin Imaging. 1997. 21:246–251.37. Weirich SD, Cotler HB, Narayana PA, Hazle JD, Jackson EF, Coupe KJ, et al. Histopathologic correlation of magnetic resonance imaging signal patterns in a spinal cord injury model. Spine. 1990. 15:630–638.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Magnetic Resonance Imaging of Traumatic Cervical Injury
- Magnetic Resonance Imaging of Acute Cervical Cord Injuries (Clinical Correlation and Prognosis)
- Diagnosis and Prognosis of Adult Post-traumatic Cervical Cord Injury Without Radiographic Evidence of Trauma Using Magnetic Resonance Imaging
- Clinical Influence of Cervical Spinal Canal Stenosis on Neurological Outcome after Traumatic Cervical Spinal Cord Injury without Major Fracture or Dislocation
- MR Imaging of Cord Transection without Skeletal Injury: A case Report
