Effects of Long-Distance Running on Cardiac Markers and Biomarkers in Exercise-Induced Hypertension Runners: An Observational Study
- Affiliations
-
- 1Department of Rehabilitation Medicine, Inje University Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- 2Department of Clinical Laboratory Science, Shinsung University, Dangjin, Korea.
- 3Department of Sports Medicine, Soonchunhyang University, Asan, Korea.
- 4Department of Exercise Physiology, Korea National Sport University, Seoul, Korea.
- 5Department of Exercise Rehabilitation Welfare, Sungshin University - Soojung Campus, Seoul, Korea. kyj87@sungshin.ac.kr
- KMID: 2420050
- DOI: http://doi.org/10.5535/arm.2018.42.4.575
Abstract
OBJECTIVE
To investigate changes of cardiac and muscle damage markers in exercise-induced hypertension (EIH) runners before running (pre-race), immediately after completing a 100-km ultramarathon race, and during the recovery period (24, 72, and 120 hours post-race).
METHODS
In this observational study, volunteers were divided into EIH group (n=11) whose maximum systolic blood pressure was ≥210 mmHg in graded exercise testing and normal exercise blood pressure response (NEBPR) group (n=11). Their blood samples were collected at pre-race, immediately after race, and at 24, 72, and 120 hours post-race.
RESULTS
Creatine kinase (CK) and cardiac troponin I (cTnI) levels were significantly higher in EIH group than those in the NEBPR group immediately after race and at 24 hours post-race (all p < 0.05). However, lactate dehydrogenase (LDH), creatine kinase-myocardial band (CKMB), or CKMB/CK levels did not show any significant differences between the two groups in each period. N-terminal pro-brain natriuretic peptide (NT-proBNP) levels were significantly higher in EIH group than those in NEBPR group immediately after race and at 24 and 72 hours post-race (all p < 0.05). A high sensitivity C-reactive protein (hs-CRP) level was significantly higher in EIH group than that in NEBPR group at 24 hours post-race (p < 0.05).
CONCLUSION
The phenomenon of higher inflammatory and cardiac marker levels in EIH group may exaggerate cardiac volume pressure and blood flow restrictions which in turn can result in cardiac muscle damage. Further prospective studies are needed to investigate the chronic effect of such phenomenon on the cardiovascular system in EIH runners.
Keyword
MeSH Terms
-
Biomarkers*
Blood Pressure
C-Reactive Protein
Cardiac Volume
Cardiovascular System
Continental Population Groups
Creatine
Creatine Kinase
Exercise Test
Humans
Hypertension*
L-Lactate Dehydrogenase
Myocardium
Observational Study*
Prospective Studies
Running*
Troponin I
Volunteers
Biomarkers
C-Reactive Protein
Creatine
Creatine Kinase
L-Lactate Dehydrogenase
Troponin I
Figure
-
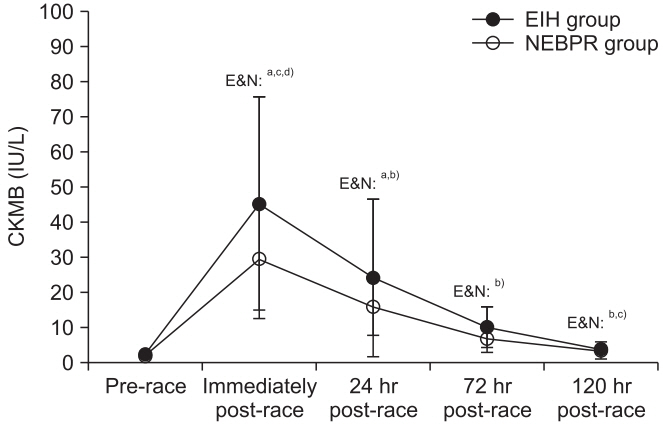
Fig. 1. Responses of CKMB to 100-km ultra-marathon race and its recovery in EIH and NEBPR groups. CK, creatine kinase; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the pre-race at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 24 hours post-race at p<0.05, d)significantly different from the 72 hours post-race at p<0.05.

Fig. 2. Responses of CKMB/CK (ratio) to 100-km ultramarathon race and its recovery in EIH and NEBPR groups. CK, creatine kinase; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the 24 hours post-race at p<0.05.
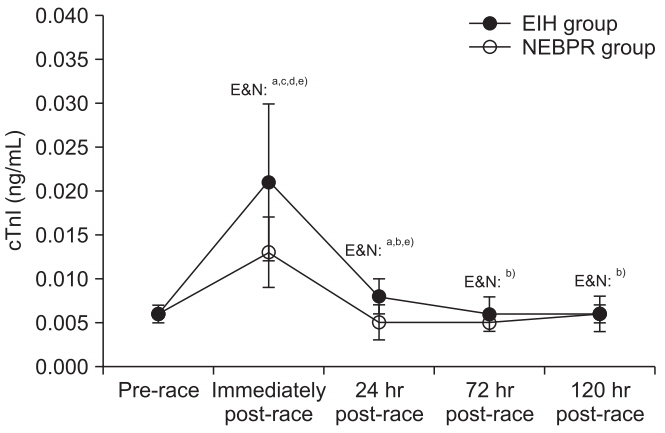
Fig. 3. Responses of cTnI to 100-km ultra-marathon race and its recovery in EIH and NEBPR groups. cTnI, cardiac troponin I; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the pre-race at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 24 hours post-race at p<0.05, d)significantly different from the 72 hours post-race at p<0.05, e)significantly different between the groups at p<0.05.
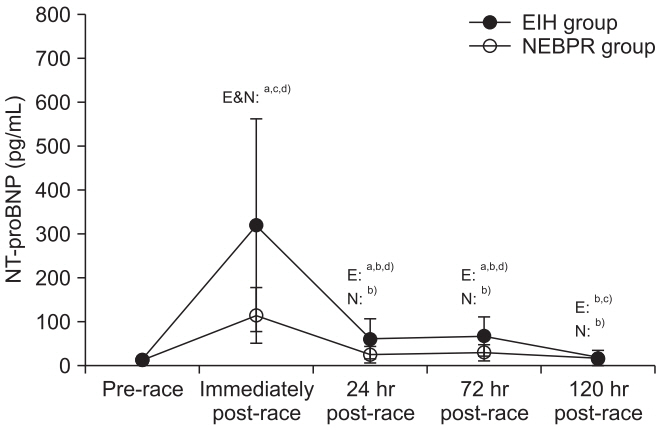
Fig. 4. Responses of NT-proBNP to 100-km ultra-marathon race and its recovery in EIH and NEBPR groups. NTproBNP, N-terminal pro B-type natriuretic peptide; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the pre-race at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 72 hours post-race at p<0.05, d)significantly different between the groups at p<0.05.
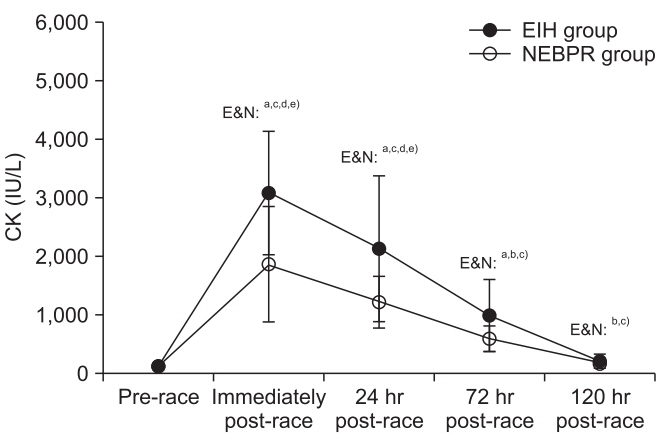
Fig. 5. Responses of CK to 100-km ultra-marathon race and its recovery in EIH and NEBPR groups. CK, creatine kinase; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the pre-race at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 24 hours post-race at p<0.05, d)significantly different from the 72 hours post-race at p<0.05, e)significantly different between the groups at p<0.05.

Fig. 6. Responses of hs-CRP to 100-km ultra-marathon race and its recovery in EIH and NEBPR groups. hsCRP, high sensitive C-reactive protein; EIHG, exerciseinduced hypertension; NEBPRG, normal exercise blood pressure response. a)Significantly different from the prerace at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 24 hours post-race at p<0.05, d)significantly different from the 72 hours post-race at p<0.05, e)significantly different between the groups at p<0.05.
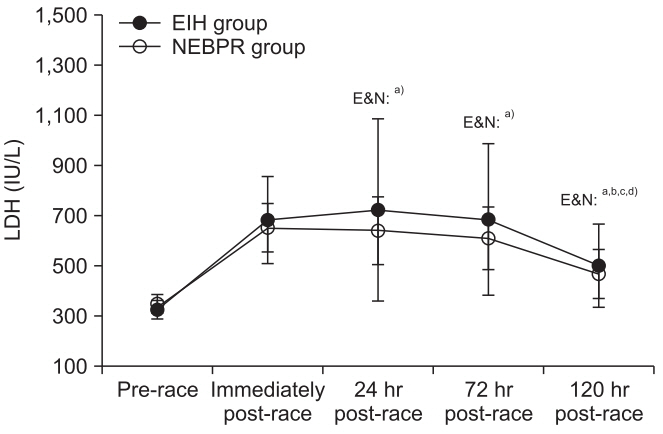
Fig. 7. Responses of LDH to 100-km ultramarathon race and its recovery in EIH and NEBPR groups. LDH, lactate dehydrogenase; EIH, exercise-induced hypertension; NEBPR, normal exercise blood pressure response. a)Significantly different from the pre-race at p<0.05, b)significantly different from immediately post-race at p<0.05, c)significantly different from the 24 hours post-race at p<0.05, d)significantly different from the 72 hours postrace at p<0.05.
Reference
-
1. Scharhag J, Herrmann M, Urhausen A, Haschke M, Herrmann W, Kindermann W. Independent elevations of N-terminal pro-brain natriuretic peptide and cardiac troponins in endurance athletes after prolonged strenuous exercise. Am Heart J. 2005; 150:1128–34.
Article2. Scott JM, Esch BT, Shave R, Warburton DE, Gaze D, George K. Cardiovascular consequences of completing a 160-km ultramarathon. Med Sci Sports Exerc. 2009; 41:26–34.
Article3. Roth HJ, Leithauser RM, Doppelmayr H, Doppelmayr M, Finkernagel H, von Duvillard SP, et al. Cardiospecificity of the 3rd generation cardiac troponin T assay during and after a 216 km ultra-endurance marathon run in Death Valley. Clin Res Cardiol. 2007; 96:359–64.
Article4. Tchou I, Margeli A, Tsironi M, Skenderi K, Barnet M, Kanaka-Gantenbein C, et al. Growth-differentiation factor-15, endoglin and N-terminal pro-brain natriuretic peptide induction in athletes participating in an ultramarathon foot race. Biomarkers. 2009; 14:418–22.
Article5. Kim YJ, Shin YO, Lee JB, Lee YH, Shin KA, Kim AC, et al. The effects of running a 308 km ultra-marathon on cardiac markers. Eur J Sport Sci. 2014; 14 Suppl 1:S92–7.
Article6. Lavie CJ, Arena R, Swift DL, Johannsen NM, Sui X, Lee DC, et al. Exercise and the cardiovascular system: clinical science and cardiovascular outcomes. Circ Res. 2015; 117:207–19.7. Lavie CJ, Lee DC, Sui X, Arena R, O’Keefe JH, Church TS, et al. Effects of running on chronic diseases and cardiovascular and all-cause mortality. Mayo Clin Proc. 2015; 90:1541–52.
Article8. Scharhag J, George K, Shave R, Urhausen A, Kindermann W. Exercise-associated increases in cardiac biomarkers. Med Sci Sports Exerc. 2008; 40:1408–15.
Article9. Legaz-Arrese A, George K, Carranza-Garcia LE, Munguia-Izquierdo D, Moros-García T, Serrano-Ostariz E. The impact of exercise intensity on the release of cardiac biomarkers in marathon runners. Eur J Appl Physiol. 2011; 111:2961–7.
Article10. Serrano-Ostariz E, Terreros-Blanco JL, Legaz-Arrese A, George K, Shave R, Bocos-Terraz P, et al. The impact of exercise duration and intensity on the release of cardiac biomarkers. Scand J Med Sci Sports. 2011; 21:244–9.11. Kim YJ, Kim CH, Shin KA, Kim AC, Lee YH, Goh CW, et al. Cardiac markers of EIH athletes in ultramarathon. Int J Sports Med. 2012; 33:171–6.
Article12. Kim YJ, Shin YO, Lee YH, Jee HM, Shin KA, Goh CW, et al. Effects of marathon running on cardiac markers and endothelin-1 in EIH athletes. Int J Sports Med. 2013; 34:777–82.
Article13. Lauer MS, Levy D, Anderson KM, Plehn JF. Is there a relationship between exercise systolic blood pressure response and left ventricular mass? The Framingham Heart Study. Ann Intern Med. 1992; 116:203–10.14. Singh JP, Larson MG, Manolio TA, O’Donnell CJ, Lauer M, Evans JC, et al. Blood pressure response during treadmill testing as a risk factor for new-onset hypertension. The Framingham heart study. Circulation. 1999; 99:1831–6.15. Kjeldsen SE, Mundal R, Sandvik L, Erikssen G, Thaulow E, Erikssen J. Exercise blood pressure predicts cardiovascular death and myocardial infarction. Blood Press Monit. 1997; 2:147–53.16. Kurl S, Laukkanen JA, Rauramaa R, Lakka TA, Sivenius J, Salonen JT. Systolic blood pressure response to exercise stress test and risk of stroke. Stroke. 2001; 32:2036–41.
Article17. Gibbons RJ, Balady GJ, Beasley JW, Bricker JT, Duvernoy WF, Froelicher VF, et al. ACC/AHA guidelines for exercise testing: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). Circulation. 1997; 96:345–54.18. Clarkson PM. Exertional rhabdomyolysis and acute renal failure in marathon runners. Sports Med. 2007; 37:361–3.
Article19. Pearson JR, Carrea F. Evaluation of the clinical usefulness of a chemiluminometric method for measuring creatine kinase MB. Clin Chem. 1990; 36:1809–11.
Article20. Shin KA, Park KD, Ahn J, Park Y, Kim YJ. Comparison of changes in biochemical markers for skeletal muscles, hepatic metabolism, and renal function after three types of long-distance running: observational study. Medicine (Baltimore). 2016; 95:e3657.21. Adams JE 3rd, Bodor GS, Davila-Roman VG, Delmez JA, Apple FS, Ladenson JH, et al. Cardiac troponin I: a marker with high specificity for cardiac injury. Circulation. 1993; 88:101–6.
Article22. McNeil PL, Terasaki M. Coping with the inevitable: how cells repair a torn surface membrane. Nat Cell Biol. 2001; 3:E124–9.
Article23. Scharhag J, Urhausen A, Schneider G, Herrmann M, Schumacher K, Haschke M, et al. Reproducibility and clinical significance of exercise-induced increases in cardiac troponins and N-terminal pro brain natriuretic peptide in endurance athletes. Eur J Cardiovasc Prev Rehabil. 2006; 13:388–97.
Article24. Herrmann M, Scharhag J, Miclea M, Urhausen A, Herrmann W, Kindermann W. Post-race kinetics of cardiac troponin T and I and N-terminal pro-brain natriuretic peptide in marathon runners. Clin Chem. 2003; 49:831–4.
Article25. Wilson M, O’Hanlon R, Prasad S, Oxborough D, Godfrey R, Alpendurada F, et al. Biological markers of cardiac damage are not related to measures of cardiac systolic and diastolic function using cardiovascular magnetic resonance and echocardiography after an acute bout of prolonged endurance exercise. Br J Sports Med. 2011; 45:780–4.
Article26. Serrano-Ostariz E, Legaz-Arrese A, Terreros-Blanco JL, Lopez-Ramon M, Cremades-Arroyos D, Carranza-Garcia LE, et al. Cardiac biomarkers and exercise duration and intensity during a cycle-touring event. Clin J Sport Med. 2009; 19:293–9.27. Shave RE, Dawson E, Whyte G, George K, Ball D, Gaze DC, et al. Evidence of exercise-induced cardiac dysfunction and elevated cTnT in separate cohorts competing in an ultra-endurance mountain marathon race. Int J Sports Med. 2002; 23:489–94.
Article28. Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapid measurement of Btype natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002; 347:161–7.
Article29. Wilson MF, Sung BH, Pincomb GA, Lovallo WR. Exaggerated pressure response to exercise in men at risk for systemic hypertension. Am J Cardiol. 1990; 66:731–6.
Article30. Kim HJ, Lee YH, Kim CK. Changes in serum cartilage oligomeric matrix protein (COMP), plasma CPK and plasma hs-CRP in relation to running distance in a marathon (42.195 km) and an ultra-marathon (200 km) race. Eur J Appl Physiol. 2009; 105:765–70.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rhabdomyolysis and Changes of Biochemical Markers in the Long-Distance Runners
- Effects of Ultra-Marathon Running on Pro-inflammatory, Anti-inflammatory and Endothelial Function Factors in Athletes with Exercise-induced Hypertension
- Cardiovascular Adaptation and Side Effects in Middle-Aged Marathoners
- Comparison of Changes in Glucose and Lipid Parameters Associated with Three Types of Long-Distance Running
- Effects of Super-Ultramarathon Races (622 km) on Cardiac Bio-Markers and Markers of Muscle Damage
