J Korean Neurosurg Soc.
2018 Jul;61(4):450-457. 10.3340/jkns.2017.0606.004.
Endosaccular Treatment of Very Large and Giant Intracranial Aneurysms with Parent Artery Preservation: Single Center Experience with Long Term Follow-up
- Affiliations
-
- 1Department of Neurosurgery, Inje University Haeundae Paik Hospital, Busan, Korea.
- 2Department of Neurosurgery, Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea. medifirst@pusan.ac.kr
- 3Department of Diagnostic Radiology, Medical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea.
- 4Department of Neurosurgery, Kosin University Gaspel Hospital, Busan, Korea.
- KMID: 2417320
- DOI: http://doi.org/10.3340/jkns.2017.0606.004
Abstract
OBJECTIVE
Very large (20-25 mm) and giant (≥25 mm) intracranial aneurysms have an extremely poor natural course, and treatment of these aneurysms remains a challenge for endovascular and surgical strategies. This study was undertaken to describe our experiences of endosaccular treatment of very large and giant intracranial aneurysms with parent artery preservation.
METHODS
From January 2005 to October 2016, twenty-four very large or giant aneurysms in 24 patients were treated by endosaccular coil embolization with parent artery preservation. Nine (37.5%) aneurysms were ruptured and 15 were unruptured, and of these 15, 11 were symptomatic cases and 4 were incidentally discovered. The cohort comprised 17 women and 7 men of mean age 58.5 years (range, 26-82). Mean aneurysm size was 26.0 mm (range, 20-39) and 13 of the 24 aneurysms were giant.
RESULTS
Immediate angiographic results were complete occlusion in nine (37.5%) cases, remnant neck in six (25.0%), and remnant sac in nine (37.5%). Overall procedural related morbidity and mortality rates were 12.5% and 4.2%, respectively. Angiographic follow-up was available in 16 patients (66.7%). Mean and median follow-up periods were 27.2 (range, 2-77) and 10.5 months, respectively. In 12 cases (12/16, 75%) stable occlusion was achieved, four cases (4/16, 25%) had recanalized, and two of these were retreated with additional coiling. At clinical follow-up of the nine ruptured cases, three patients (33.3%) achieved a good clinical outcome (Glasgow outcome scale [GOS] score of 4 or 5), two (22.2%) a poor outcome (GOS score of 2 or 3), and four patients (44.4%) expired (GOS 1). On the other hand, of the 15 unruptured cases, 13 patients (86.7%) achieved a good clinical outcome (GOS 4 or 5), one patient a poor outcome (GOS score of 2 or 3), and one patient expired (GOS 1).
CONCLUSION
The present study shows endosaccular treatment of very large or giant intracranial aneurysms with parent artery preservation is both feasible and effective with acceptable morbidity and mortality.
MeSH Terms
Figure
-
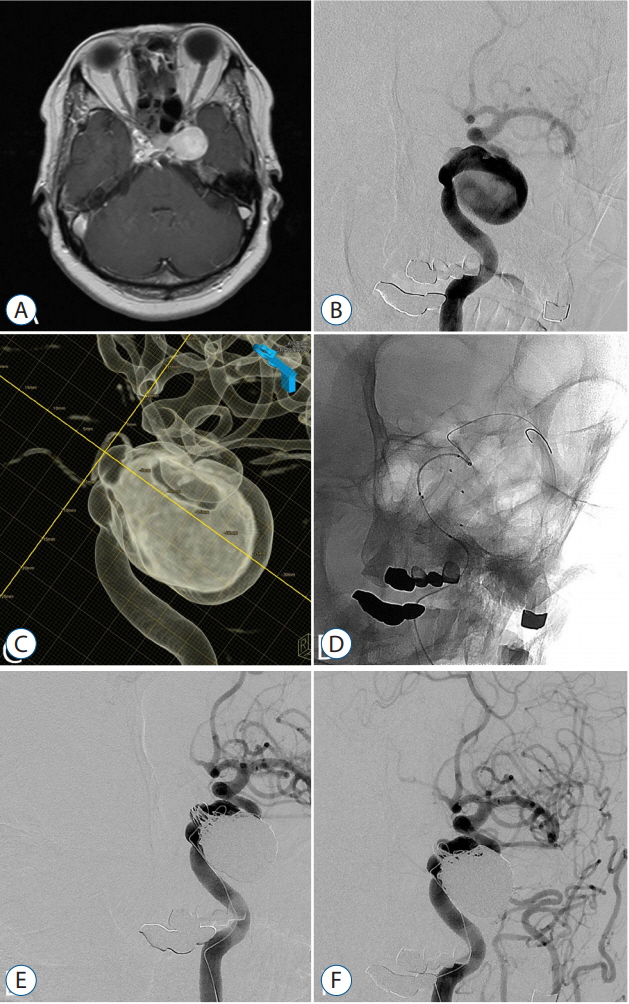
Fig. 1. A 58-year old woman with left 6th cranial nerve palsy patient. A : A pre-procedural axial T1-weighted magnetic resonance image showing a intracranial aneur ysm. B : A lef t internal carotid arter y (ICA) angiography. C : A 3-dementional reconstruction image showing a giant aneurysm arising from left cavernous segment ICA. D : The aneurysm was coiled by the multiple catheters with stent. E : A post-procedural angiography showing small remnant neck of the aneurysm with parent artery preservation. F : Seven months follow-up angiography showing stable occlusion of the aneurysm.
Reference
-
References
1. Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G, et al. Pipeline for uncoilable or failed aneurysms: results from a multicenter clinical trial. Radiology. 267:858–868. 2013.
Article2. Becske T, Potts MB, Shapiro M, Kallmes DF, Brinjikji W, Saatci I, et al. Pipeline for uncoilable or failed aneurysms: 3-year follow-up results. J Neurosurg. 127:81–88. 2017.
Article3. Brinjikji W, Murad MH, Lanzino G, Cloft HJ, Kallmes DF. Endovascular treatment of intracranial aneurysms with flow diverters: a meta-analysis. Stroke. 44:442–447. 2013.
Article4. Chalouhi N, Tjoumakaris S, Gonzalez LF, Dumont AS, Starke RM, Hasan D, et al. Coiling of large and giant aneurysms: complications and longterm results of 334 cases. AJNR Am J Neuroradiol. 35:546–552. 2014.
Article5. el-Chalouhi N, Jabbour PM, Tjoumakaris SI, Starke RM, Dumont AS, Liu H, et al. Treatment of large and giant intracranial aneurysms: cost comparison of flow diversion and traditional embolization strategies. World Neurosurg. 82:696–701. 2014.
Article6. Gao X, Liang G, Li Z, Wei X, Cao P. A single-centre experience and follow-up of patients with endovascular coiling of large and giant intracranial aneurysms with parent artery preservation. J Clin Neurosci. 19:364–369. 2012.
Article7. Gruber A, Killer M, Bavinzski G, Richling B. Clinical and angiographic results of endosaccular coiling treatment of giant and very large intracranial aneurysms: a 7-year, single-center experience. Neurosurgery. 45:793–803. discussion 803-804. 1999.
Article8. Ha SW, Jang SJ. Clinical analysis of giant intracranial aneurysms with endovascular embolization. J Cerebrovasc Endovasc Neurosurg. 14:22–28. 2012.
Article9. Hauck EF, Welch BG, White JA, Replogle RE, Purdy PD, Pride LG, et al. Stent/coil treatment of very large and giant unruptured ophthalmic and cavernous aneurysms. Surg Neurol. 71:19–24. discussion 24. 2009.
Article10. Jahromi BS, Mocco J, Bang JA, Gologorsky Y, Siddiqui AH, Horowitz MB, et al. Clinical and angiographic outcome after endovascular management of giant intracranial aneurysms. Neurosurgery. 63:662–674. discussion 674-675. 2008.
Article11. Kallmes DF, Hanel R, Lopes D, Boccardi E, Bonafe A, Cekirge S, et al. International retrospective study of the pipeline embolization device: a multicenter aneurysm treatment study. AJNR Am J Neuroradiol. 36:108–115. 2015.
Article12. Kodama N, Suzuki J. Surgical treatment of giant aneurysms. Neurosurg Rev. 5:155–160. 1982.
Article13. Leung GK, Tsang AC, Lui WM. Pipeline embolization device for intracranial aneurysm: a systematic review. Clin Neuroradiol. 22:295–303. 2012.
Article14. Li MH, Li YD, Fang C, Gu BX, Cheng YS, Wang YL, et al. Endovascular treatment of giant or very large intracranial aneurysms with different modalities: an analysis of 20 cases. Neuroradiology. 49:819–828. 2007.
Article15. Peerless SJ, Drake CG. Treatment of giant cerebral aneurysms of the anterior circulation. Neurosurg Rev. 5:149–154. 1982.
Article16. Raymond J, Gentric JC, Darsaut TE, Iancu D, Chagnon M, Weill A, et al. Flow diversion in the treatment of aneurysms: a randomized care trial and registry. J Neurosurg. 127:454–462. 2017.
Article17. Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 32:1998–2004. 2001.
Article18. Sluzewski M, Menovsky T, van Rooij WJ, Wijnalda D. Coiling of very large or giant cerebral aneurysms: long-term clinical and serial angiographic results. AJNR Am J Neuroradiol. 24:257–262. 2003.19. Sundt TM Jr, Piepgras DG. Surgical approach to giant intracranial aneurysms. Operative experience with 80 cases. J Neurosurg. 51:731–742. 1979.20. UCAS Japan Investigators, Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med. 366:2474–2482. 2012.
Article21. van Rooij WJ, Sluzewski M. Endovascular treatment of large and giant aneurysms. AJNR Am J Neuroradiol. 30:12–18. 2009.
Article22. van Rooij WJ, Sluzewski M, van der Laak C. Flow diverters for unruptured internal carotid artery aneurysms: dangerous and not yet an alternative for conventional endovascular techniques. AJNR Am J Neuroradiol. 34:3–4. 2013.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular management of large and giant intracranial aneurysms: Experience from a tertiary care neurosurgery institute in India
- Surgical Management of Large and Giant Aneurysm
- Giant Fusiform Aneurysm by Circumferential Wrapping with Sutures-Reinforcement
- Giant vertebral artery aneurysms presenting acutely with WFNS grade five subarachnoid haemorrhage, report of 4 cases treated with endovascular or surgical proximal parent artery occlusion achieving good functional outcome
- Salvage flow diverter stent across the posterior communicating artery for persistent retrograde filling of a giant internal carotid artery aneurysm after parent vessel occlusion
