Salvage flow diverter stent across the posterior communicating artery for persistent retrograde filling of a giant internal carotid artery aneurysm after parent vessel occlusion
- Affiliations
-
- 1Department of Radiology, King Fahad Medical City, Riyadh, Saudi Arabia
- 2Department of Neurosurgery, King Abdulaziz Speciality Hospital, Taif, Saudi Arabia
- 3Department of Adult Neurosurgery, National Neuroscience Institute, King Fahad Medical City, Riyadh, Saudi Arabia
- KMID: 2517025
- DOI: http://doi.org/10.7461/jcen.2021.E2020.09.002
Abstract
- Giant internal carotid artery (ICA) aneurysms are complex vascular lesions which are difficult to treat with open as well as endovascular surgery. Parent vessel occlusion is a well-established treatment option for such aneurysms. However, there have been a few reported cases of ruptured aneurysms related to the persistent retrograde filling after parent vessel occlusion. We report a case which highlights the usage of the flow diverter stent as a potential treatment strategy for the management of retrograde filling of aneurysms. A 54-year-old female was found to have a giant left ICA aneurysm on a brain magnetic resonance imaging during workup for headaches. She underwent occlusion of the left ICA proximal to the aneurysm using multiple coils. However, follow up angiograms after 6 months and 2 years demonstrated persistent retrograde filling of the left ICA aneurysm through the posterior communicating (PCOM) artery. Eventually, she was successfully treated with a flow diverter stent across the PCOM artery into the distal ICA. Follow up angiogram after 6 months showed patent flow in the PCOM artery and the distal ICA. with complete occlusion of the aneurysm. Using a flow diverter stent after insufficient parent vessel occlusion for giant intracranial aneurysms may be a feasible treatment option and an addition to the neurovascular treatment armamentarium.
Keyword
Figure
-
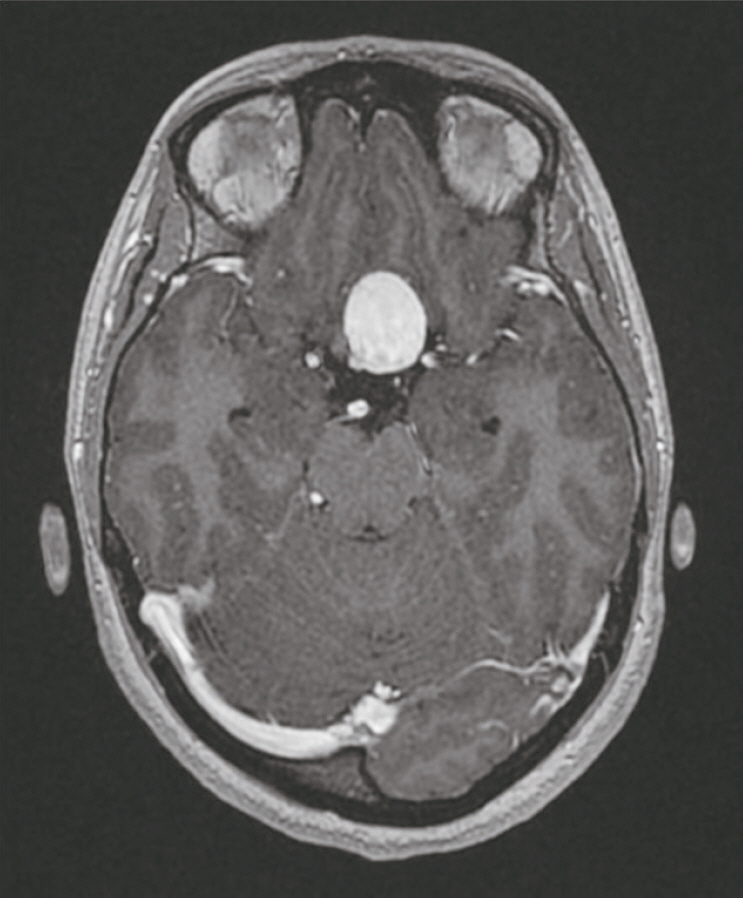
Fig. 1. MRI scan with contrast demonstrating a giant aneurysm arising from the para-ophthalmic segment of the left ICA. MRI, magnetic resonance imaging; ICA, internal carotid artery.

Fig. 2. Initial angiogram (A) AP and (B) Lateral views show large left ICA paraphthalmic aneurysm. AP, anteroposterior; ICA, internal carotid artery.

Fig. 3. (A) Balloon occlusion test left ICA with balloon inflated in left ICA and angiogram from the right ICA showing brisk filling of the left anterior and middle cerebral artery through a patent anterior communicating artery. (B) Native AP image demonstrating multiple coils used for occlusion of distal left ICA. ICA, internal carotid artery.
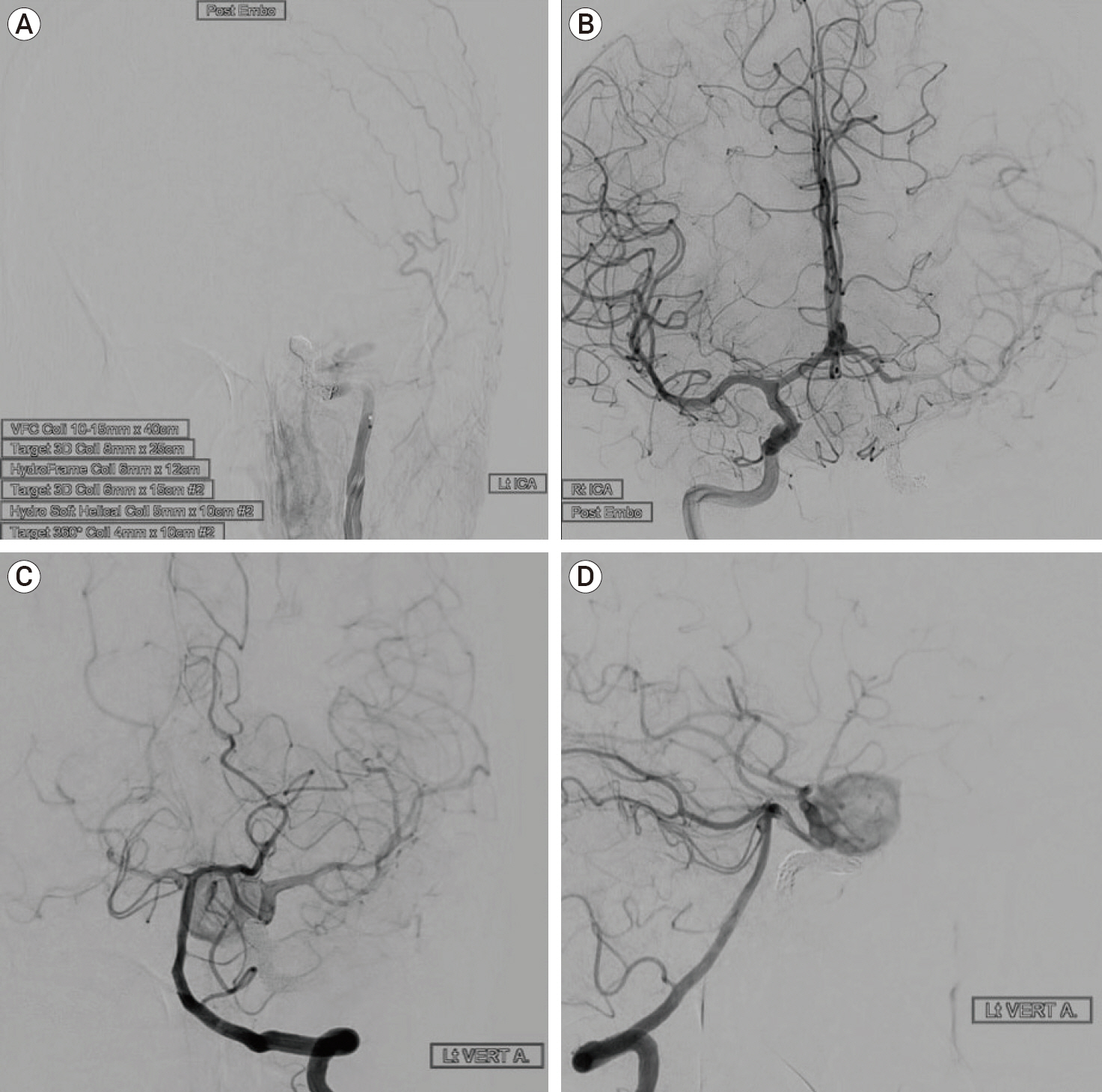
Fig. 4. (A) Left ICA AP angiogram demonstrating multiple coils causing occlusion of the distal left ICA with no antegrade filling of the left ICA aneurysm. (B) Right ICA AP angiogram post occlusion of the left ICA shows brisk filling of the left anterior and middle cerebral artery through a patent anterior communicating artery. (C, D) Left vertebral artery AP and Lateral views angiogram shows retrograde filling of the left ICA para-ophthalmic aneurysm after occlusion of left ICA. ICA, internal carotid artery; AP, anteroposterior.
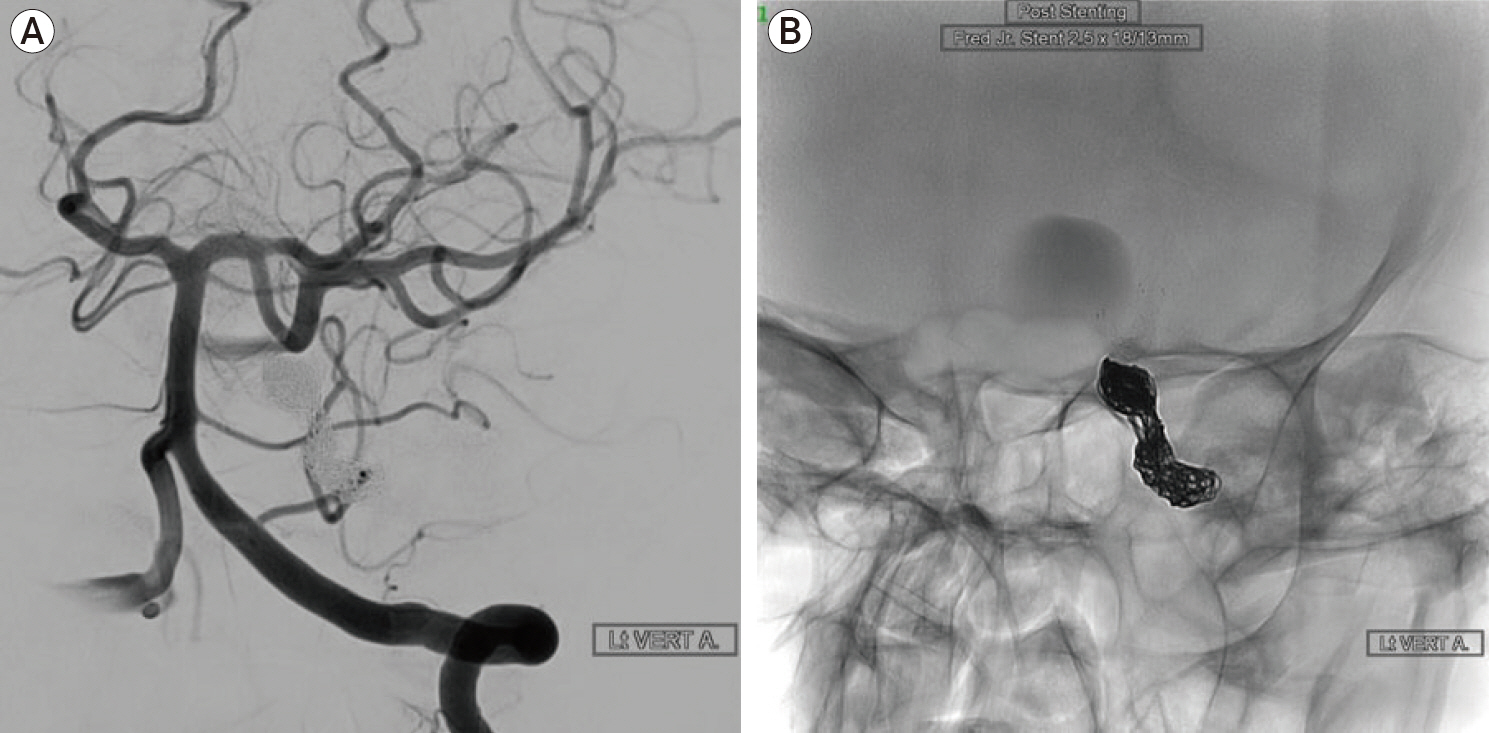
Fig. 5. (A) Oblique left vertebral angiogram demonstrates filling of the left ICA aneurysm through a patent left PCOM artery. (B) Oblique native image demonstrating the flow diverter stent across the PCOM artery into the distal left ICA terminating below the carotid terminus. ICA, internal carotid artery; PCOM, posterior communicating.
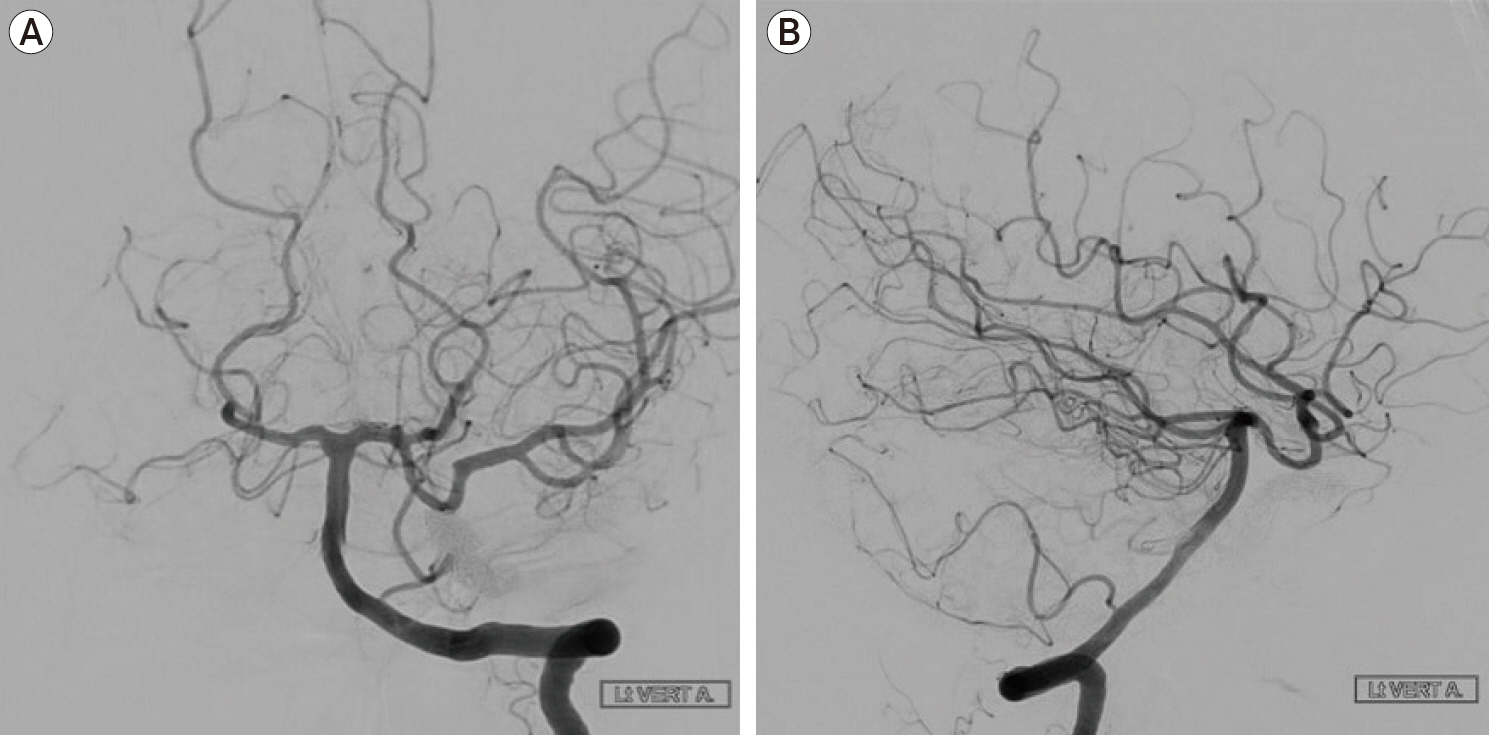
Fig. 6. Six months follow up AP and lateral angiogram of the left vertebral artery demonstrating patent PCOM artery aneurysm with no residual filling of the left ICA aneurysm. AP, anteroposterior. PCOM, posterior communicating; ICA, internal carotid artery.
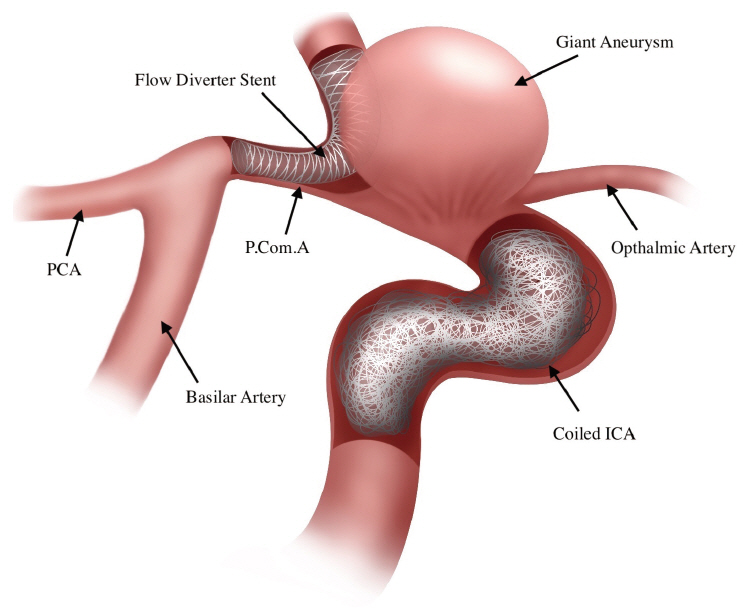
Fig. 7. An illustration showing parent ICA occlusion with placement of flow diverter stent across the left PCOM artery into the distal left ICA. ICA, internal carotid artery; PCOM, posterior communicating.
Reference
-
1. Adeeb N, Griessenauer CJ, Shallwani H, Shakir H, Foreman PM, Moore JM, et al. Pipeline embolization device in treatment of 50 unruptured large and giant aneurysms. World Neurosurg. 2017; Sep. 105:232–7.
Article2. Bechan RS, Majoie CB, Sprengers ME, Peluso JP, Sluzewski M, Van Rooij WJ. Therapeutic internal carotid artery occlusion for large and giant aneurysms: A single center cohort of 146. Am J Neuroradiol. 2016; 37(1):125–9.3. Becske T, Kallmes DF, Saatci I, McDougall CG, Szikora I, Lanzino G, et al. Pipeline for uncoilable or failed aneurysms: results from a multicenter clinical trial. Radiology. 2013; Jun. 267(3):858–68.
Article4. Cui L, Peng Q, Ha W, Zhou D, Xu Y. Parent artery occlusion for intracranial aneurysms. Interv Neuroradiol. 2009; Sep. 15(3):309–15.
Article5. Gurian JH, Viñuela F, Gobin YP, Waston VE, Duckwiler GR, Gulielmi G. Aneurysm rupture after parent vessel sacrifice: treatment with Guglielmi detachable coil embolization via retrograde catheterization: case report. Neurosurgery. 1995; Dec. 37(6):1216–20. discussion 1220-1.6. Sluzewski M, Menovsky T, van Rooij WJ, Wijnalda D. Coiling of very large or giant cerebral aneurysms: long-term clinical and serial angiographic results. AJNR Am J Neuroradiol. 2003; Feb. 24(2):257–62.7. Solomon RA, Fink ME, Pile-Spellman J. Surgical management of unruptured intracranial aneurysms. J Neurosurg. 1994; Mar. 80(3):440–6.
Article8. van Rooij WJ, Sluzewski M, Metz NH, Nijssen PC, Wijnalda D, Rinkel GJ, et al. Carotid balloon occlusion for large and giant aneurysms: evaluation of a new test occlusion protocol. Neurosurgery. 2000; Jul. 47(1):116–21. discussion 122.
Article9. Vincent F, Weill A, Roy D, Raymond J, Guilbert F. Carotid ophthalmic aneurysm rupture after parent vessel occlusion. AJNR Am J Neuroradiol. 2005; Jun-Jul. 26(6):1372–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Kinking of Flow Diverter in a Giant Wide-Necked Supraclinoid Internal Carotid Artery Aneurysm
- Fusiform “True” Posterior Communicating Artery Aneurysm with Basilar Artery Occlusion: A Case Report
- Symptomatic Post Endarterectomy Common Carotid Artery Pseudoaneurysm Treated with Combination of Flow Diverter Implantation and Carotid Stenting
- Retreatment of a recurrent giant aneurysm of the internal carotid artery after treatment with a flow-diverting stent
- Intracranial Aneurysm Associated with Aplasia of the Internal Cartoid Artery
