Extensive Pituitary Apoplexy after Chemotherapy in a Patient with Metastatic Breast Cancer
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- 2Department of Pathology, National Cancer Center, Graduate School of Cancer Science and Policy, Goyang, Korea.
- 3Department of Cancer Control, National Cancer Center, Graduate School of Cancer Science and Policy, Goyang, Korea. nsghs@ncc.re.kr
- KMID: 2410237
- DOI: http://doi.org/10.14791/btrt.2018.6.e7
Abstract
- Surgery, anticoagulation therapy, pregnancy, and hormone treatments, such as bromocriptine, are well-characterized precipitating factors for pituitary apoplexy. However, whether cytotoxic chemotherapy for systemic cancer could cause pituitary apoplexy has not been investigated. Here, we present a case of a 41-year-old woman who developed a severe headache with decreased visual acuity after intravenous cytotoxic chemotherapy to treat metastatic breast cancer. Preoperative neuroimaging revealed pituitary adenoma with necrosis. Operative findings and pathologic examination concluded extensive necrosis with a small intratumoral hemorrhage in a pre-existing pituitary adenoma. We reviewed two additional previously published cases of pituitary apoplexy after systemic chemotherapy and suggest that cytotoxic chemotherapy may induce pituitary apoplexy.
MeSH Terms
Figure
-
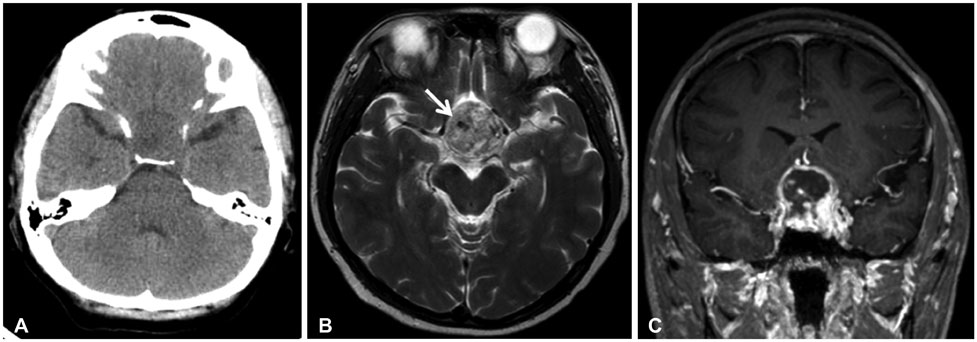
Fig. 1 Preoperative neuro-images. (A) Pre-operative brain computed tomography scan demonstrating a lobulated, contoured, low-density lesion on the widened sella. There was no evidence of either intracranial or intratumoral hemorrhage. Pre-operative magnetic resonance imaging of T2 axial (B) and T1 weighted (C), gadolinium-enhancement, coronal views showing lobulated, contoured, large, mixed solid and necrotic masses with spotty intratumoral hemorrhage (white arrow) and suprasellar extension.
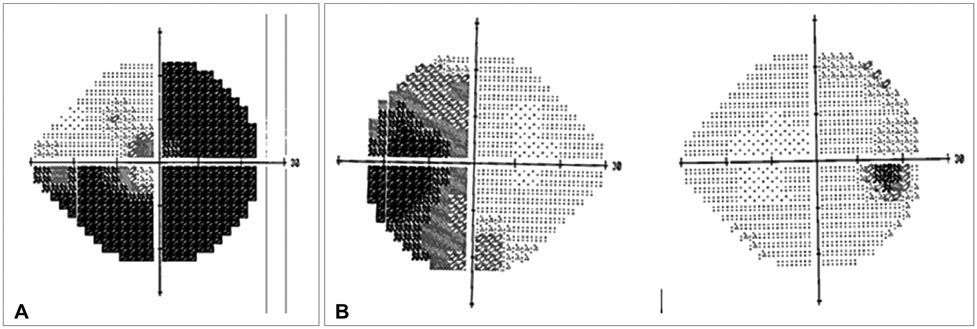
Fig. 2 Pre- and post-operative visual field examinations. A: Visual field tests were not possible on the left eye. Lateral and inferior medial three-quadrant anopsia was found preoperatively. B: Postoperative 2-month visual field test revealed nearly complete recovery of the right eye and left-eye temporal hemianopsia.
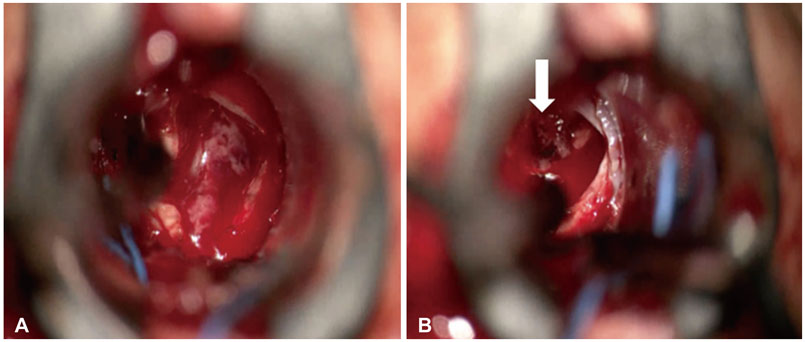
Fig. 3 Intra-operative picture showing necrotic material flowing out after dura incision (A) and a mass with blood clot (white arrow) (B).

Fig. 4 Pituitary adenoma showing varying degree of necrosis (hematoxylin and eosin staining, ×400). Some areas retain papillary tumor configuration which is readily discernable as pituitary adenoma, although the tumor shows pyknotic nuclei and acidophilic cytoplasm (A) and complete necrosis of tumor cells in this area, showing ghosty cells (B).
Reference
-
1. Semple PL, Jane JA Jr, Laws ER Jr. Clinical relevance of precipitating factors in pituitary apoplexy. Neurosurgery. 2007; 61:956–961.
Article2. Guerrero-Pérez F, Marengo AP, Planas-Vilaseca A, Flores-Escobar V, Villabona-Artero C. Pituitary apoplexy induced by triptorelin in patient with prostate cancer. Endocrinol Nutr. 2015; 62:411–412.
Article3. Chng E, Dalan R. Pituitary apoplexy associated with cabergoline therapy. J Clin Neurosci. 2013; 20:1637–1643.
Article4. Silberstein L, Johnston C, Bhagat A, Tibi L, Harrison J. Pituitary apoplexy during induction chemotherapy for acute myeloid leukaemia. Br J Haematol. 2008; 143:151.
Article5. Davies JS, Rees DA, Evans LM, Scanlon MF. Pituitary apoplexy following combination chemotherapy-a case report. Endocr Relat Cancer. 1998; 5:151–153.6. Biousse V, Newman NJ, Oyesiku NM. Precipitating factors in pituitary apoplexy. J Neurol Neurosurg Psychiatry. 2001; 71:542–545.
Article
