A Systematic Review and Meta-analysis of Randomized Controlled Trials Comparing Surgical versus Conservative Treatments for Acute Undisplaced or Minimally-Displaced Scaphoid Fractures
- Affiliations
-
- 1Imam Muhammad Ibn Saud Islamic University, College of Medicine, Riyadh, Saudi Arabia. turki--aj@hotmail.com
- 2Al-Faisal Private University, College of Medicine, Riyadh, Saudi Arabia.
- 3California State University, College of Science, Los Angeles, CA, USA.
- 4Department of Plastic and Reconstructive Surgery, Security Forces Hospital, Riyadh, Saudi Arabia.
- KMID: 2405484
- DOI: http://doi.org/10.4055/cios.2018.10.1.64
Abstract
- BACKGROUND
Surgical and conservative methods have been reported by various studies for high rates of fracture union and subsequent regain of function among patients with undisplaced or minimally-displaced scaphoid fractures. Hence, this study aims to analyze the best available evidence to comprehend the relative benefits and risks of these therapeutic options.
METHODS
A systematic search of the literature from different databases and search engines was performed with strict eligibility criteria to obtain the highest quality of evidence. All randomized controlled trials delineating the outcomes of surgical versus conservative treatments for acute undisplaced or minimally-displaced scaphoid fractures were included and then evaluated using scoring tools: Cochrane risk of bias tool and PEDro scale. Data were pooled using random-effects models with standard mean differences for continuous outcomes and risk ratios for dichotomous variables.
RESULTS
The search yielded 339 potentially related articles, further trimmed down to eight studies based on the eligibility criteria. The meta-analysis revealed that surgical treatment resulted in significantly better functional outcomes than conservative treatment. Furthermore, surgery resulted in the prevention of delayed union of fractures and reduction of time needed to return to work.
CONCLUSIONS
While four studies reported advantages of surgical treatment, evidence was insufficient to provide a definitive conclusion that surgery is a better option. Due to the significant limitations with respect to certain variables, the superiority of one method to the other could not be established.
Keyword
Figure
-
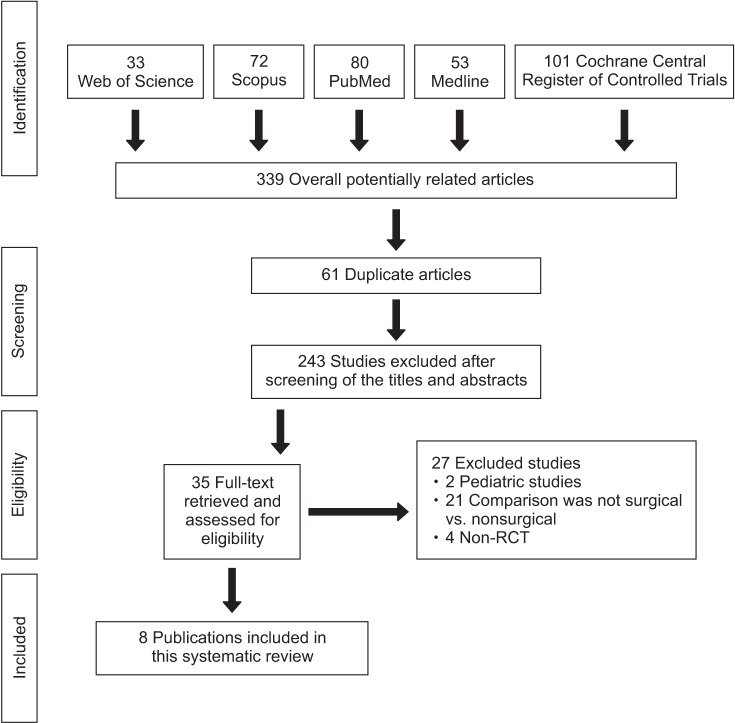
Fig. 1 Flowchart of selection of studies and specific reasons for exclusion from the present meta-analysis. RCT: randomized controlled trial.
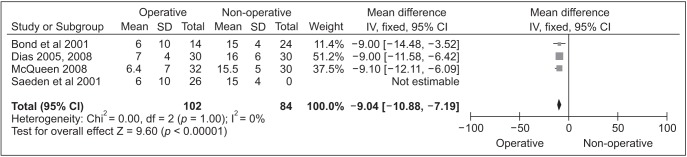
Fig. 2 Forest plot for the weighted mean difference estimate for the time to return to work weighting given to the trial in the overall pooled estimate, taking into account the number of participants and the amount of interstudy variation (heterogeneity) rhombus, and combined effect size. SD: standard deviation, CI: confidence interval.
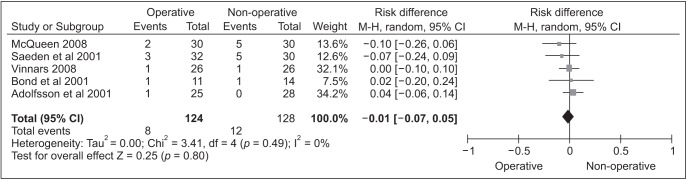
Fig. 3 Forest plot for the risk ratio estimate for the assessment of overall complication rate. CI: confidence interval.
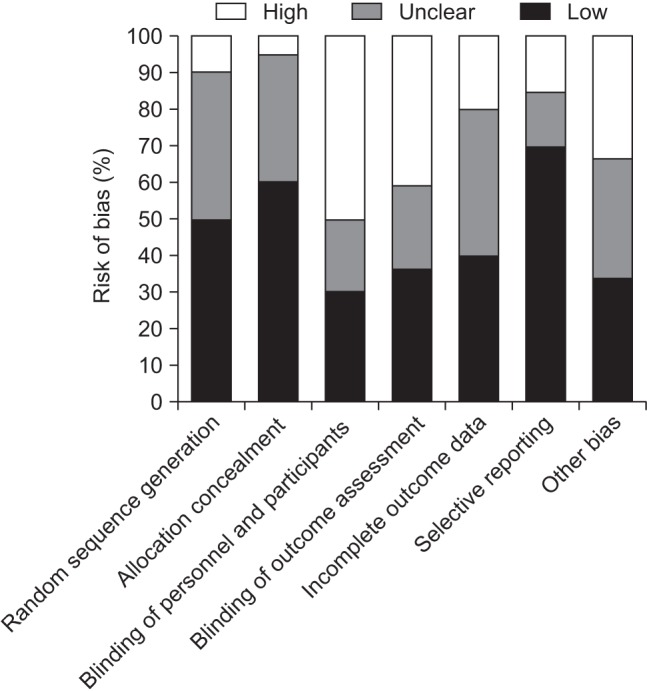
Fig. 4 Risk of bias graph: authors' judgements about each risk of bias item presented as percentages across all included studies.

Fig. 5 Sensitivity analysis and publication bias analysis of the meta-analysis. The figure shows the influence of individual study on summary risk ratio (RR) computed by omitting each study in turn. The vertical axis indicates the overall RR and the two vertical axes indicate the 95% confidence interval (CI). Every circle indicates the pooled RR when the study is omitted in this meta-analysis. The two ends of the dotted lines represent the 95% CI.
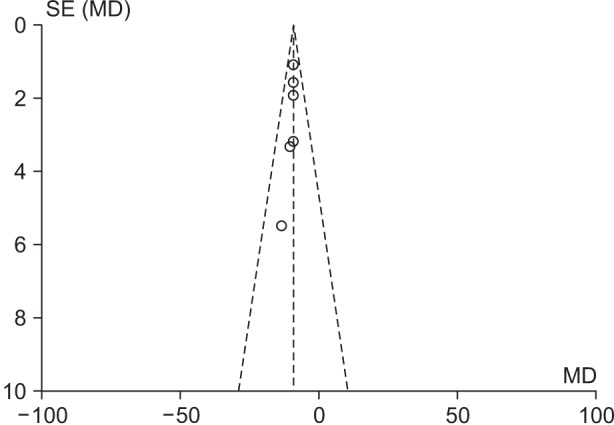
Fig. 6 Begg's funnel plot for publication bias in the selection of studies. The horizontal axis represents the log risk ratio (RR) and the vertical axis indicates the standard error (SE) of the log RR. The vertical line and the sloping lines represent the effects summary RR and the expected 95% confidence interval for a given SE. Each circle represents the eight studies. The symmetrical appearance of the funnel means that there is no publication bias in the selection of the studies included in this metaanalysis. MD: mean difference.
Reference
-
1. Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg. 1999; 33(4):423–426. PMID: 10614752.
Article2. Buijze GA, Doornberg JN, Ham JS, Ring D, Bhandari M, Poolman RW. Surgical compared with conservative treatment for acute nondisplaced or minimally displaced scaphoid fractures: a systematic review and meta-analysis of randomized controlled trials. J Bone Joint Surg Am. 2010; 92(6):1534–1544. PMID: 20516332.3. Paulus MC, Braunstein J, Merenstein D, et al. Variability in orthopedic surgeon treatment preferences for nondisplaced scaphoid fractures: a cross-sectional survey. J Orthop. 2016; 13(4):337–342. PMID: 27436923.
Article4. Bond CD, Shin AY, McBride MT, Dao KD. Percutaneous screw fixation or cast immobilization for nondisplaced scaphoid fractures. J Bone Joint Surg Am. 2001; 83(4):483–488. PMID: 11315775.
Article5. Clementson M, Jorgsholm P, Besjakov J, Thomsen N, Bjorkman A. Conservative treatment versus arthroscopic-assisted screw fixation of scaphoid waist fractures: a randomized trial with minimum 4-year follow-up. J Hand Surg Am. 2015; 40(7):1341–1348. PMID: 25913660.6. McQueen MM, Gelbke MK, Wakefield A, Will EM, Gaebler C. Percutaneous screw fixation versus conservative treatment for fractures of the waist of the scaphoid: a prospective randomised study. J Bone Joint Surg Br. 2008; 90(1):66–71. PMID: 18160502.7. Vinnars B, Pietreanu M, Bodestedt A, Ekenstam Fa, Gerdin B. Nonoperative compared with operative treatment of acute scaphoid fractures: a randomized clinical trial. J Bone Joint Surg Am. 2008; 90(6):1176–1185. PMID: 18519309.8. Dias JJ, Dhukaram V, Abhinav A, Bhowal B, Wildin CJ. Clinical and radiological outcome of cast immobilisation versus surgical treatment of acute scaphoid fractures at a mean follow-up of 93 months. J Bone Joint Surg Br. 2008; 90(7):899–905. PMID: 18591600.
Article9. Adolfsson L, Lindau T, Arner M. Acutrak screw fixation versus cast immobilisation for undisplaced scaphoid waist fractures. J Hand Surg Br. 2001; 26(3):192–195. PMID: 11386765.
Article10. Dias JJ, Wildin CJ, Bhowal B, Thompson JR. Should acute scaphoid fractures be fixed? A randomized controlled trial. J Bone Joint Surg Am. 2005; 87(10):2160–2168. PMID: 16203878.11. Saeden B, Tornkvist H, Ponzer S, Hoglund M. Fracture of the carpal scaphoid: a prospective, randomised 12-year follow-up comparing operative and conservative treatment. J Bone Joint Surg Br. 2001; 83(2):230–234. PMID: 11284571.12. Higgins JP, Altman DG, editors. Cochrane handbook for systematic reviews of interventions. ver. 5.1.0. Chichester, UK: John Wiley & Sons;2011. p. 190–193.13. Anz AW, Bushnell BD, Bynum DK, Chloros GD, Wiesler ER. Pediatric scaphoid fractures. J Am Acad Orthop Surg. 2009; 17(2):77–87. PMID: 19202121.
Article14. Ring D, Jupiter JB, Herndon JH. Acute fractures of the scaphoid. J Am Acad Orthop Surg. 2000; 8(4):225–231. PMID: 10951111.
Article15. Mack GR, Kelly JP, Lichtman DM. Scaphoid non-union. In : Lichtman DM, Alexander AH, editors. The wrist and its disorders. Philadelphia, PA: WB Saunders;1997. p. 234–267.16. Markiewitz AD, Stern PJ. Current perspectives in the management of scaphoid nonunions. Instr Course Lect. 2005; 54:99–113. PMID: 15948438.17. Mack GR, Bosse MJ, Gelberman RH, Yu E. The natural history of scaphoid non-union. J Bone Joint Surg Am. 1984; 66(4):504–509. PMID: 6707028.
Article18. Shen L, Tang J, Luo C, Xie X, An Z, Zhang C. Comparison of operative and non-operative treatment of acute undisplaced or minimally-displaced scaphoid fractures: a meta-analysis of randomized controlled trials. PLoS One. 2015; 10(5):e0125247. PMID: 25942316.
Article19. Armstrong CA, Oldham JA. A comparison of dominant and non-dominant hand strengths. J Hand Surg Br. 1999; 24(4):421–425. PMID: 10473148.
Article20. Bohannon RW. Grip strength: a summary of studies comparing dominant and nondominant limb measurements. Percept Mot Skills. 2003; 96(3 Pt 1):728–730. PMID: 12831245.
Article21. Incel NA, Ceceli E, Durukan PB, Erdem HR, Yorgancioglu ZR. Grip strength: effect of hand dominance. Singapore Med J. 2002; 43(5):234–237. PMID: 12188074.22. Grewal R, Suh N, MacDermid JC. Is casting for non-displaced simple scaphoid waist fracture effective? A CT based assessment of union. Open Orthop J. 2016; 10:431–438. PMID: 27708739.
Article23. Dias JJ, Taylor M, Thompson J, Brenkel IJ, Gregg PJ. Radiographic signs of union of scaphoid fractures: an analysis of inter-observer agreement and reproducibility. J Bone Joint Surg Br. 1988; 70(2):299–301. PMID: 3346310.
Article24. Singh HP, Forward D, Davis TR, Dawson JS, Oni JA, Downing ND. Partial union of acute scaphoid fractures. J Hand Surg Br. 2005; 30(5):440–445. PMID: 16006021.
Article25. Dias JJ, Singh HP. Displaced fracture of the waist of the scaphoid. J Bone Joint Surg Br. 2011; 93(11):1433–1439. PMID: 22058291.
Article26. Yin ZG, Zhang JB, Kan SL, Wang P. Treatment of acute scaphoid fractures: systematic review and meta-analysis. Clin Orthop Relat Res. 2007; 460:142–151. PMID: 17310931.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Nonoperative Treatment for Undisplaced Scaphoid Fracture
- Effect of intracanal cryotherapy on postendodontic pain: a systematic review and meta-analysis of randomized controlled trials
- Introduction to systematic review and meta-analysis
- A Diagnosis and Treatment of Carpal Scaphoid Fractures
- A Treatment of Carpal Scaphoid Fracture
