J Korean Orthop Assoc.
2009 Dec;44(6):668-674. 10.4055/jkoa.2009.44.6.668.
Nonoperative Treatment for Undisplaced Scaphoid Fracture
- Affiliations
-
- 1Department of Orthopedic Surgery, St. Mary's Hospital, Catholic University Medical College, Seoul, Korea. sw.song@catholic.ac.kr
- KMID: 2186294
- DOI: http://doi.org/10.4055/jkoa.2009.44.6.668
Abstract
- PURPOSE
We wanted to evaluate the results of nonoperative treatment for acute, undisplaced, stable scaphoid fracture.
MATERIALS AND METHODS
We retrospectively reviewed 24 cases of acute undisplaced scaphoid fracture that were treated at our department from May 1998 to January 2008. The immobilization method was a long or short arm cast. Flexion-extension exercise was permitted during the period of the short arm cast, but pronation-supination motion was prohibited. After the removal of the cast, active and passive range of motion exercise was started immediately. The result was assessed by the Maudsley scale.
RESULTS
The twenty four cases were undisplaced or minimally displaced fracture (10 cases of Herbert type A1, 3 cases of A2 and 11 cases of B2) according to the Mayo classification. The average duration of immobilization was 7.16 weeks. According to the Maudsley scale, 19 cases had an excellent result and 4 cases had a good result. One case had a complication of scapho-lunate dissociation.
CONCLUSION
We recommend conservative treatment with cast immobilization as the first treatment of choice for acute undisplaced scaphoid fracture.
Figure
-

Fig. 1 (A, B) Plain radiographs of 22-year-old female patient showed fracture at the waist of scaphoid. (C, D) After thumb-spica cast for 6 weeks, plain radiographs showed bony union.
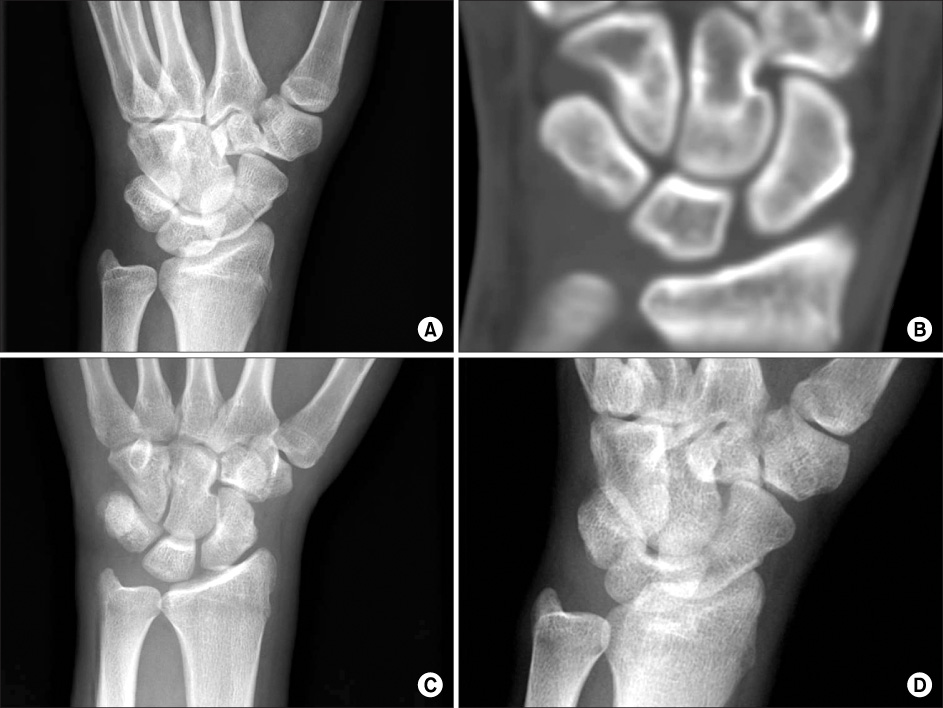
Fig. 2 (A, B) Plain radiograph and computed tomogram showed scaphoid fracture, Herbert type B2. (C, D) After thumb-spica cast for 7 weeks, the follow-up plain X-ray film showed bony union of the undisplaced fracture fragment.
Reference
-
1. Hove LM. Epidemiology of scaphoid fractures in Bergen, Norway. Scand J Plast Reconstr Surg Hand Surg. 1999. 33:423–426.
Article2. Sherman SB, Greenspan A, Norman A. Osteonecrosis of the distal pole of the carpal scaphoid following fracture--a rare complication. Skeletal Radio. 1983. 9:189–191.3. Bunker TD, McNamee PB, Scott TD. The Herbert screw for scaphoid fractures. A multicentre study. J Bone Joint Surg Br. 1987. 69:631–634.
Article4. Cooney WP, Dobyns JH, Linscheid RL. Fractures of the scaphoid: a rational approach to management. Clin Orthop Relat Res. 1980. 149:90–97.5. Inoue G, Shionoya K. Herbert screw fixation by limited access for acute fractures of the scaphoid. J Bone Joint Surg Br. 1997. 79:418–421.
Article6. Rettig ME, Kozin SH, Cooney WP. Open reduction and internal fixation of acute displaced scaphoid waist fractures. J Hand Surg Am. 2001. 26:271–276.
Article7. Saedén B, Törnkvist H, Ponzer S, Höglund M. Fracture of the carpal scaphoid. A prospective, randomised 12-year follow-up comparing operative and conservative treatment. J Bone Joint Surg Br. 2001. 83:230–234.8. Adolfsson L, Lindau T, Arner M. Acutrak screw fixation versus cast immobilisation for undisplaced scaphoid waist fractures. J Hand Surg Br. 2001. 26:192–195.
Article9. Bond CD, Shin AY, McBride MT, Dao KD. Percutaneous screw fixation or cast immobilization for nondisplaced scaphoid fractures. J Bone Joint Surg Am. 2001. 83:483–488.10. Dias JJ, Wildin CJ, Bhowal B, Thompson JR. Should acute scaphoid fractures be fixed? A randomized controlled trial. J Bone Joint Surg Am. 2005. 87:2160–2168.11. Dias JJ, Brenkel IJ, Finlay DB. Patterns of union in fractures of the waist of the scaphoid. J Bone Joint Surg Br. 1989. 71:307–310.12. Ford DJ, Khoury G, el-Hadidi S, Lunn PG, Burke FD. The Herbert screw for fractures of the scaphoid. A review of results and technical difficulties. J Bone Joint Surg Br. 1987. 69:124–127.
Article13. Gellman H, Caputo RJ, Carter V, Aboulafia A, McKay M. Comparison of short and long thumb-spica casts for non-displaced fractures of the carpal scaphoid. J Bone Joint Surg Am. 1989. 71:354–357.
Article14. Leslie IJ, Dickson RA. The fractured carpal scaphoid. Natural history and factors influencing outcome. J Bone Joint Surg Br. 1981. 63:225–230.
Article15. King RJ, Mackenney RP, Elnur S. Suggested method for closed treatment of fractures of the carpal scaphoid: hypothesis supported by dissection and clinical practice. J R Soc Med. 1982. 75:860–867.16. Maudsley RH, Chen SC. Screw fixation in the management of the fractured carpal scaphoid. J Bone Joint Surg Br. 1972. 54:432–441.
Article17. Eddeland A, Eiken O, Hellgren E, Ohlsson NM. Fractures of the scaphoid. Scand J Plast Reconstr Surg. 1975. 9:234–239.
Article18. McLaughlin HL, Parkes JC 2nd. Fracture of the carpal navicular (scaphoid) bone: gradations in therapy based upon pathology. J Trauma. 1969. 9:311–319.19. Kozin SH. Internal fixation of scaphoid fractures. Hand Clin. 1997. 13:573–586.
Article20. Szabo RM, Manske D. Displaced fractures of the scaphoid. Clin Orthop Relat Res. 1988. 230:30–38.
Article21. Sanders WE. Evaluation of the humpback scaphoid by computed tomography in the longitudinal axial plane of the scaphoid. J Hand Surg Am. 1988. 13:182–187.
Article22. Verdan C. The role of the anterior radiocarpal ligament in fractures of the scaphoid carpus; therapeutic deductions. Z Unfallmed Berufskr. 1954. 47:294–297.23. O'Brien L, Herbert T. Internal fixation of acute scaphoid fractures: a new approach to treatment. Aust N Z J Surg. 1985. 55:387–389.24. Skirven T, Trope J. Complications of immobilization. Hand Clin. 1994. 10:53–61.
Article25. Dias JJ, Bhowal B, Wildin CJ, Thompson JR. Assessing the outcome of disorders of the hand. Is the patient evaluation measure reliable, valid, responsive and without bias? J Bone Joint Surg Br. 2001. 83:235–240.26. Yin ZG, Zhang JB, Kan SL, Wang P. Treatment of acute scaphoid fractures: systematic review and meta-analysis. Clin Orthop Relat Res. 2007. 460:142–151.27. Vinnars B, Pietreanu M, Bodestedt A, Ekenstam F, Gerdin B. Nonoperative compared with operative treatment of acute scaphoid fractures. A randomized clinical trial J Bone Joint Surg Am. 2008. 90:1176–1185.
Article28. Huene DR. Primary internal fixation of carpal navicular fractures in the athlete. Am J Sports Med. 1979. 7:175–177.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of the Scaphoid Fracture
- Treatment of Carpal Scaphoid Fracture
- Scaphoid Fractures and Nonunions: Recent Trends of Treatment
- Comparison of Distal Radius Fractures with or without Scaphoid Fractures
- Rupture of the Extensor Pollicis Longus after Fracture of the Distal end of the Radius: Report of 3 cases
