Improved Imaging of the Cervico-Thoracic Junction in Computed Tomography
- Affiliations
-
- 1Department of Radiology, Ansan Hospital, Korea University Medical Center, Ansan, Korea. ksu45112@chollian.net
- 2Department of Radiologic Science, College of Health Sciences, Korea University, Seoul, Korea.
- 3Department of Radiology, Anam Hospital, Korea University Medical Center, Seoul, Korea.
- 4Divisions of Medical Sensor, Samil-Pharm. Co., Seoul, Korea.
- 5Department of Display and Semiconductor Physics, Chungnam, Korea.
Abstract
- PURPOSE
To reduce beam hardening artifacts caused by the shoulder joint, we explored new and unique methods to improve the quality of images, such as varying the injection site and changing the position of patients (swimmers position). MATERIALS AND METHODS: Fifth-four patients underwent neck CT examinations performed in routine and swimmers position and with a 64-slice MDCT scanner in spiral scanning. To examine the difference due to the injection sites of contrast material, subjects were divided into right- and left-side groups. For the evaluation of images, we carried out a subjective and objective assessment based on radiologists' ratings and noise measurement. RESULTS: Images of the lower neck in the swimmers position exhibited less hardening and streak artifacts. The subjective and objective evaluations showed that the swimmers position received higher rating by radiologists and had lower noise level than that of routine position. The swimmers position was the most effective for the diagnosis of the cervico-thoracic junction area. As for the injection site, we obtained better images by an injection of contrast material in the right arm than in the left. CONCLUSION: CT examination of the lower neck in the swimmers position may improve the quality of image and the effectiveness of diagnosis. The injection of a contrast material to the right side rather than the left side reduced foreign body artifacts.
MeSH Terms
Figure
-

Fig. 1 Topography of the neck in the routine position (Left) and swimmers position (Right).

Fig. 2 The selected region used to assess CT number and noise, namely, the spinal cord, body of the first thoracic spine, and scalene muscle.
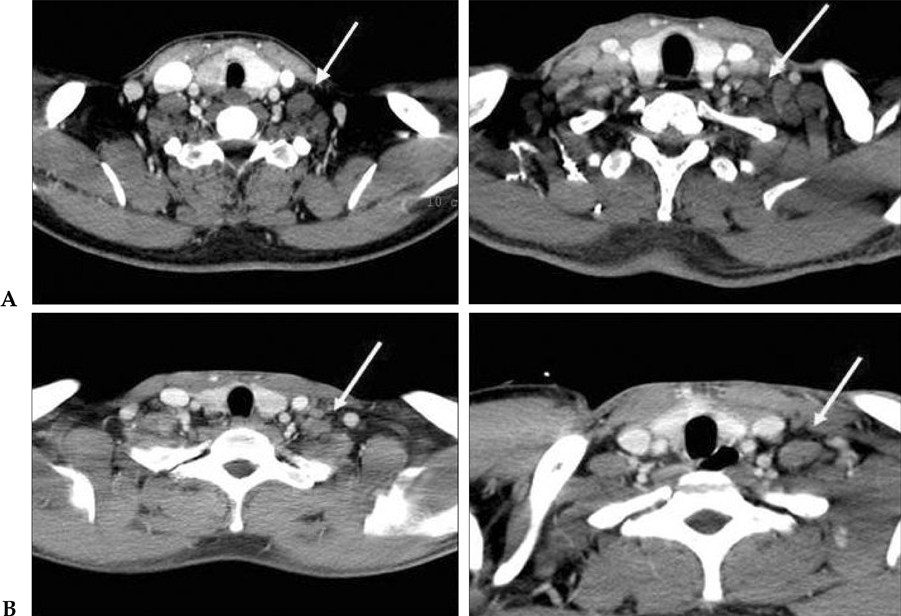
Fig. 3 Images of the sthenic (left) and hypersthenic (right) in (A) the routine position and (B) swimmers position. The streak artifacts (arrow indicated) shown in Figure (A) disappeared in the swimmers position in both cases.
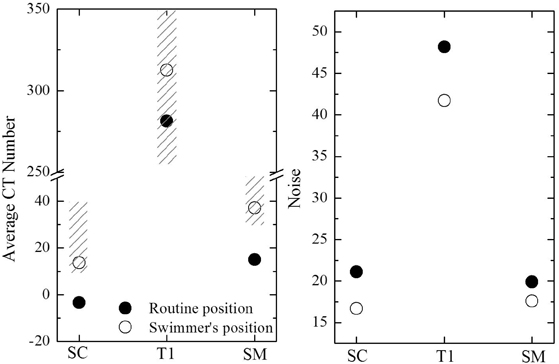
Fig. 4 CT number and noise assessment at the spinal cord, body of first thoracic spine, and scalene muscle. The shaded area represents a tolerable CT number; that is, Hounsfield units in the respective body tissues and fluids. 20
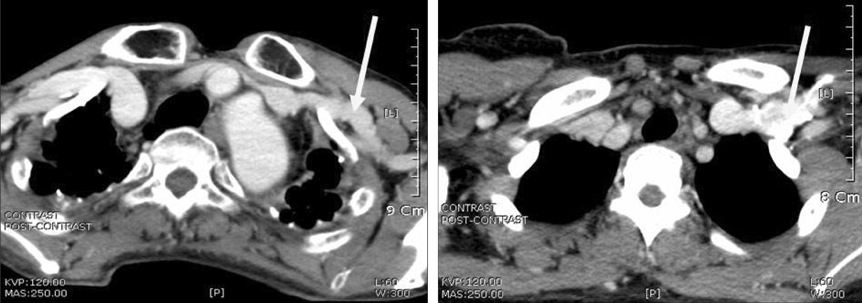
Fig. 5 Comparison of images according to injection site (left: right arm injection; right: left arm injection). The right figure shows artifacts that originated from the slow blood flow rate that resulted in acute curvature of the left subclavian vein.

Fig. 6 Routine position (left) and swimmers position (right). There is a break in symmetry in the swimmers position.
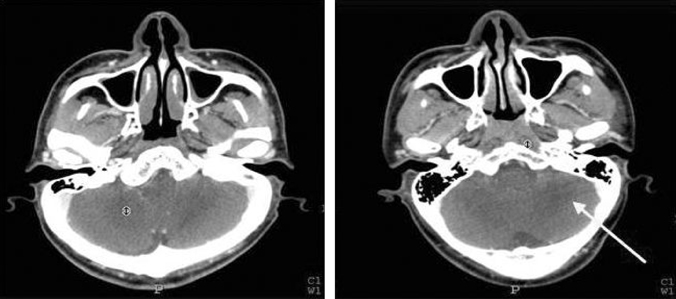
Fig. 7 Streak artifacts within the cerebellum (left: routine position, right: swimmers position).
Reference
-
1. Rothenberg LN. Seibert JA, Barnes CT, Gould RG, editors. CT dose assessment. Specifications and acceptance testing in quality control of diagnostic x-ray equipment. 1994. New York, NY: American Association of Physicists in Medicine;Monograph 20.2. Hounsfield GN. Computerized transverse axial scanning (tomography). I. Description of system. Br J Radiol. 1973. 46:1016–1022.
Article3. Fullerton GD, Zagzebski JA. Medical physics of CT and Ultrasound: Tissue imaging and Characterization, Medical physics monograph No. 6. 1980. New York: American Institute of physics (for the AAPM);717.4. Siewerdsen JH, Jaffray DA. Cone-beam computed tomography with a flat-panel imager: magnitude and effects of x-ray scatter. Med Phys. 2001. 28:220–231.
Article5. Jarry G, Graham SA, Moseley DJ, Jaffray DJ, Siewerdsen JH, Verhaegen F. Characterization of scattered radiation in kV CBCT images using Monte Carlo simulations. Med Phys. 2006. 33:4320–4329.
Article6. Glover GH. Compton scatters effects in CT reconstruction. Med Phys. 1982. 9:860–867.7. Brooks RA, Di Chiro G. Beam hardening in x-ray reconstructive tomography. Phys Med Biol. 1976. 21:390–398.
Article8. McDavid WD, Waggener RG, Payne WH, Dennis MJ. Correction for spectral artifacts in cross-sectional reconstruction from x-rays. Med Phys. 1977. 4:54–57.
Article9. Link TM, Berning W, Scherf S, Joosten U, Joist A, Engelke K, et al. CT of metal implants: reduction of artifacts using an extended CT scale technique. J Comput Assist Tomogr. 2000. 24:165–172.10. Hinderling T, Rüegsegger P, Anliker M, Dietschi C. Computed tomography reconstruction from hollow projections: an application to in vivo evaluation of artificial hip joints. J Comput Assist Tomogr. 1979. 3:52–57.11. Kalender WA, Hebel R, Ebersberger J. Reduction of CT artifacts caused by metallic implants. Radiology. 1987. 164:576–577.
Article12. Nassi M, Brody WR, Medoff BP, Macovski A. Iterative reconstruction-reprojection: an algorithm for limited data cardiac-computed tomography. IEEE Trans Biomed Eng. 1982. 29:333–341.
Article13. Wang G, Snyder DL, Vannier MW. Local computed tomography via iterative deblurring. Scanning. 1996. 18:582–588.
Article14. Mott DJ, Zheng GL, Eddleston B. The removal of a "cupping" artefact from brain images produced by the EMI 7070 CT scanner. Br J Radiol. 1985. 58:873–880.15. Soltanian-Zadeh H, Windham JP, Soltanianzadeh J. CT artifact correction: An image processing approach. SPIE. 1996. 2710:477–485.16. Kane AG, Reilly KC, Murphy TF. Swimmer's CT: improved imaging of the lower neck and thoracic inlet. Am J Neuroradiol. 2004. 25:859–862.17. Gisbert VL, Hollerman JJ, Ney AL, Rockswold GL, Ruiz E, Jacobs DM, et al. Incidence and diagnosis of C7-T1 fractures and subluxations in multiple-trauma patients: evaluation of the advanced trauma life support guidelines. Surgery. 1989. 106:702–709.18. American College of Surgeons Committee on Trauma. Advanced trauma life support program for physicians. Instructor manual. 1984. Chicago: American College of Surgeons.19. Tehranzadeh J, Bonk RT, Ansari A, Mesgarzadeh M. Efficacy of limited CT for nonvisualized lower cervical spine in patients with blunt trauma. Skeletal Radiol. 1994. 23:349–352.
Article20. Wegener OH, Fassel R. Whole Body Computed Tomography. 1993. 2nd ed. Boston: Blackwell Scientific Publications.21. Lin JT, Lee JL, Lee ST. Evaluation of occult cervical spine fractures on radiographs and CT. Emerg Radiol. 2003. 10:128–134.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Flexion-distraction Injury in Cervico-thoracic Junction: A Case Report
- Supraclavicular Approach to a Lesion in the Cervico-Thoracic Junction
- The Report of 20 Cases of Craniovertebral Junction Abnormalities
- Sternum-Splitting Approach for Anterior Space-Taking Lesions in the Upper Thoracic Lesion
- MDCT Application of Thoracic Imaging
