Flexion-distraction Injury in Cervico-thoracic Junction: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Hanyang University College of Medicine, Guri, Korea. kcpark@hanyang.ac.kr
- KMID: 2209645
- DOI: http://doi.org/10.4184/jkss.2006.13.3.215
Abstract
- Injuries at the cervico-thoracic junction can be difficult to diagnose (with an incidence as high as 9% of all spinal injuries) and to stabilize, because of anatomic complexities. We report a case with that was treated with a lateral mass screw and transpedicular screw-rod fixation for a flexion-distraction injury at the cervico-thoracic junction and we present a review of the literature.
MeSH Terms
Figure
-

Fig. 1. (A-C) Anterior-posterior roentgenogram of cervico-thoracic spine shows abnormal alignment of spinous process (A). CT scan shows anterior column collapse at T4,5 ver-tebral bodies and multiple spinous process fractures at C6 to T4 with widening of inter-laminar space between T1-2 and T3-4 (B). MRI shows no cord compressive lesion but interspinous ligament injury between C6 and T4 vertebra (C). It is diagnosed flexion dis-traction injury in cervico-thoracic junction

Fig. 2. Postoperative 3D-CT scan shows good alignment of cervico-thoracic spines with good position of lateral mass screws at cervical spines and pedicle screws at thoracic spines.
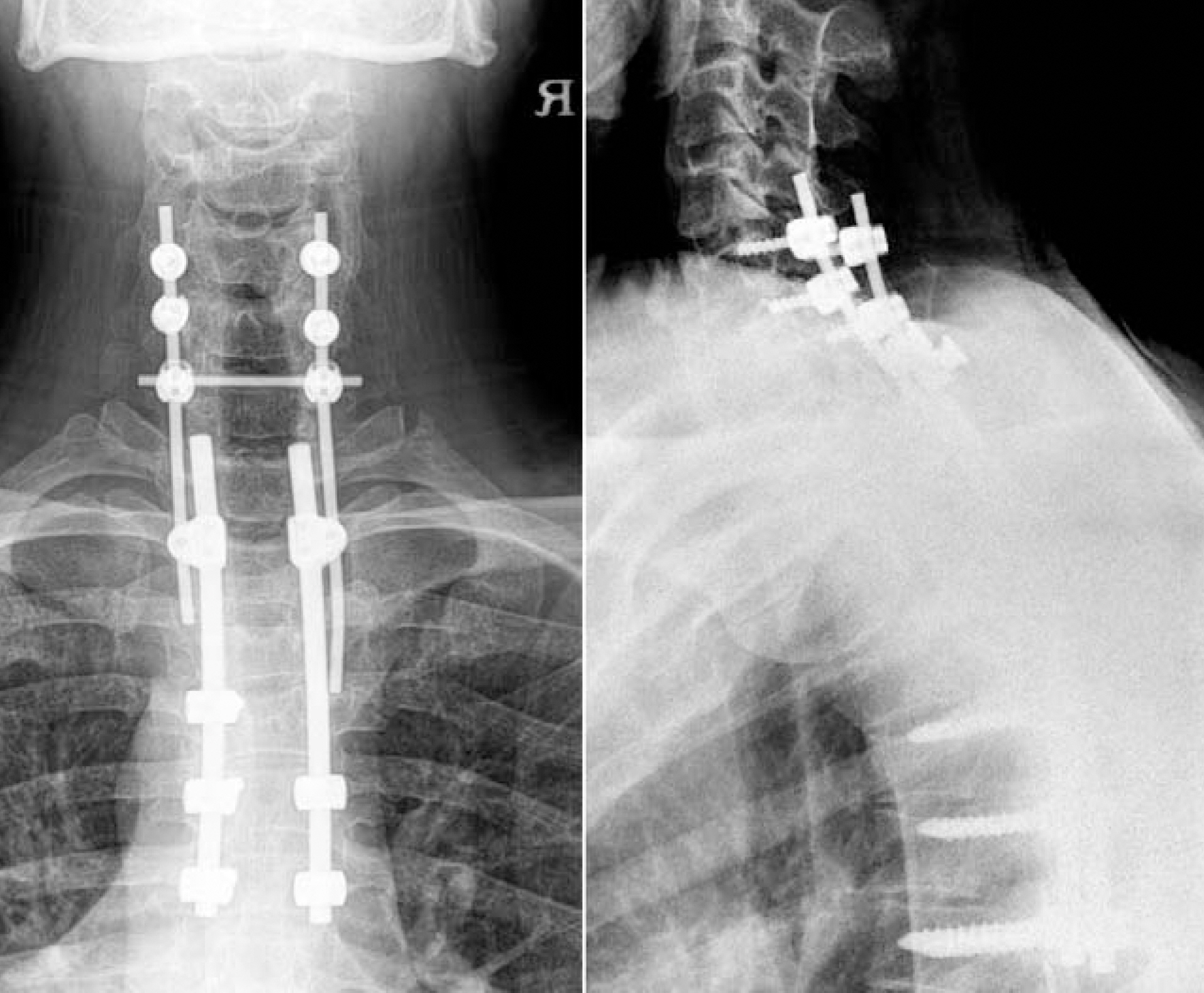
Fig. 3. With one year follow up, postoperative roentgenogram shows no breakage of instrument and change in alignment of cervico-thoracic spine.
Reference
-
01). An HS., Gordin R., Renner K. Anatomic considerations for plate-screw fixation of the cervical spine. Spine. 1991. 16(10 Suppl):S548–S551.
Article02). Sapkas G., Papadakis S., Katonis P., Roidis N., Kontakis G. Operative treatment of unstable injuries of the cervicothoracic junction. Eur Spine J. 1999. 8:279–283.
Article03). Stanescu S., Ebraheim NA., Yeasting R., Bailey AS., Jackson WT. Morphometric evaluation of the cervicothoracic junction. Practical considerations for posterior fixation of the spine. Spine. 1994. 19:2082–2088.04). Bohlman HH., Freehafer A., Dejak J. The results of treatment of acute injuries of the upper thoracic spine with paralysis. J Bone Joint Surg Am. 1985. 67:360–369.
Article05). Evans DK. Dislocations at the cervicothoracic junction. J Bone Joint Surg Br. 1983. 65:124–127.
Article06). Amin A., Saifuddin A. Fractures and dislocations of the cervicothoracic junction. J spinal Disord Tech. 2005. 18:499–505.
Article07). Kreshak JL., Kim DH., Lindsey DP., Kam AC., Panjabi MM., Yerby SA. Posterior stabilization at the cervicotho- racic junction: a biomechanical study. Spine. 2002. 27:2763–2770.08). Deen HG., Birch BD., Wharen RE., Reimer R. Lateral mass screw-rod fixation of the cervical spine: a prospective clinical series with 1-year follow-up. Spine J. 2003. 3:489–495.
Article09). Sekhon LH. Posterior cervical lateral mass screw fixation: analysis of 1026 consecutive screws in 143 patients. J Spinal Disord Tech. 2005. 18:297–303.10). Rhee JM., Kraiwattanapong C., Hutton WC. A compari-son of pedicle and lateral mass screw construct stiffnesses at the cervicothoracic junction: a biomechanical study. Spine. 2005. 30:E636–E640.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Supraclavicular Approach to a Lesion in the Cervico-Thoracic Junction
- Short Segment Fixation of Flexion-Distraction Injuries in Thoracolumbar Spines
- The Report of 20 Cases of Craniovertebral Junction Abnormalities
- Sternum-Splitting Approach for Anterior Space-Taking Lesions in the Upper Thoracic Lesion
- Delayed-Onset Leg Weakness Caused by Posterior Migration of a Herniated Disc to the Thecal Sac Mimicking Epidural Hematoma in a Flexion-Distraction Injury of the Lumbar Spine: A Case Report
