Medial Lemniscus Tract Lesion After High Voltage Electrical Injury: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Keimyung University School of Medicine, Daegu, Korea.
- 2Department of Physical Medicine and Rehabilitation, Yeungnam University College of Medicine, Daegu, Korea. hikkali@hanmail.net
- KMID: 2389492
- DOI: http://doi.org/10.5535/arm.2017.41.2.318
Abstract
- We present the case of a 33-year-old man who experienced a 10,000-V electrical shock when working with electrical wiring. He suffered third-degree burns on his scalp at the right occiput (entry wound) and on his left arm (exit would), and a second-degree burn on his left foot (exit wound). He presented with severe spasticity of both lower extremities, motor weakness with a Medical Research Council grade of 3, and sensory impairments below thoracic level 11 that included an inability to sense light touch and defects in proprioception. Initial magnetic resonance imaging (MRI) scans of his spine and brain showed no definite abnormalities. However, tractography obtained by diffusion tensor imaging of the brain showed absence of the right medial lemniscus tract. A cervical MRI scan 1 month later showed spinal cord swelling from cervical 1-5 levels, and signal changes in the lateral and posterior white matter in the axial view. After 6 months of rehabilitation, he recovered almost normal degree of motor function in his lower extremities and disappearance of spasticity. However, since the sensory impairments persisted, especially defects in proprioception, he was unable to walk independently.
MeSH Terms
Figure
-

Fig. 1 A third-degree burn on the right scalp of the patient, and skull necrosis.

Fig. 2 (A, C) A cervical spinal magnetic resonance imaging (MRI) taken 1 week after the injury reveals no specific findings, but a brain MRI shows signal changes in the right temporal lobe. (B) A cervical spine T2-weighted MRI, taken 30 days after the injury, shows swelling and signal changes from C1 to C5. (D) An axial T2-weighted image at the C2-3 level shows damage to the lateral and posterior column.
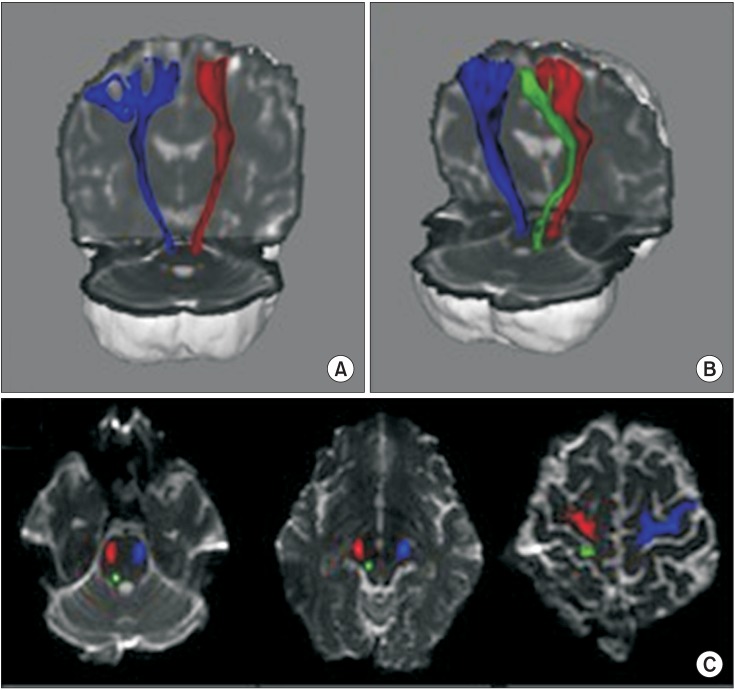
Fig. 3 Tractography of the corticospinal tract (CST) and medial lemniscus tract (ML). (A) The right CST (red) and left CST (blue) are well-connected on each anatomical level from the brain stem to the cortex. (A, B) Although the ML (green) is seen in the right hemisphere, it cannot be viewed in the left hemisphere. Both CST and right ML are properly located on the anatomical locations from cerebral cortex to pons level (C).
Reference
-
1. Arnoldo BD, Purdue GF, Kowalske K, Helm PA, Burris A, Hunt JL. Electrical injuries: a 20-year review. J Burn Care Rehabil. 2004; 25:479–484. PMID: 15534455.
Article2. Ratnayake B, Emmanuel ER, Walker CC. Neurological sequelae following a high voltage electrical burn. Burns. 1996; 22:574–577. PMID: 8909765.
Article3. Ko SH, Chun W, Kim HC. Delayed spinal cord injury following electrical burns: a 7-year experience. Burns. 2004; 30:691–695. PMID: 15475144.
Article4. Clouston PD, Sharpe D. Rapid recovery after delayed myelopathy from electrical burns. J Neurol Neurosurg Psychiatry. 1989; 52:1308.
Article5. Tun K, Cemil B, Gurcay AG, Kaptanoglu E, Sargon MF, Tekdemir I, et al. Ultrastructural evaluation of Pulsed Radiofrequency and Conventional Radiofrequency lesions in rat sciatic nerve. Surg Neurol. 2009; 72:496–500. discussion 501. PMID: 19329170.
Article6. Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TE, Johansen-Berg H, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004; 23(Suppl 1):S208–S219. PMID: 15501092.
Article7. Jang SH, Kwon HG. Anatomical location of the medial lemniscus and spinothalamic tract at the pons in the human brain: a diffusion tensor tractography study. Somatosens Mot Res. 2013; 30:206–209. PMID: 23738628.
Article8. Varghese G, Mani MM, Redford JB. Spinal cord injuries following electrical accidents. Paraplegia. 1986; 24:159–166. PMID: 3748595.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed Spinal Cord Injury Following Low Voltage Electrical Accident
- Cheiro-oral Syndrome with INO following Brainstem Infarction
- Scalp Defect, Injuries of Skull and Brain Parenchyme Caused by High Voltage Electrical Burn: A Case Report
- Transient Quadriplegia after Low-Voltage Electric Shock
- Application of Brain Computerized Tomography to High Voltage Electrical Burns
