Risk Factors for the Rupture of Bifurcation Intracranial Aneurysms Using CT Angiography
- Affiliations
-
- 1Department of Radiology, Xinqiao Hospital, Third Military Medical University, Chongqing 400037, China. xqwgxwl@163.com
- KMID: 2374163
- DOI: http://doi.org/10.3349/ymj.2016.57.5.1178
Abstract
- PURPOSE
To investigate the clinical and morphological characteristics in relation to risk of bifurcation intracranial aneurysm rupture.
MATERIALS AND METHODS
Data from 202 consecutive patients with 219 bifurcation aneurysms (129 ruptured and 90 unruptured) managed at the authors' facility between August 2011 and July 2014 were retrospectively reviewed. Based on their clinical records and CT angiographic findings, the ability of risk factors to predict aneurysm rupture was assessed using statistical methods.
RESULTS
Age, hypertension, diabetes mellitus, and cerebral atherosclerosis were negatively correlated with aneurysm rupture. Aneurysms located in the middle cerebral artery, daughter artery ratio, lateral angle ratio (LA ratio), and neck width were negatively correlated with rupture. Aneurysms located in the anterior communicating artery, irregularity, with daughter sac, depth, width, maximum size, aspect ratio (AR), depth-to-width ratio, and bottleneck factor were significantly and positively correlated with rupture. Binary logistic regression model revealed that irregular shape [odds ratio (OR) 6.598] and AR (OR 3.507) strongly increased the risk of bifurcation aneurysm rupture, while age (OR 0.434), cerebral atherosclerosis (OR 0.125), neck width (OR 0.771), and LA ratio (OR 0.267) were negatively correlated with rupture (p<0.05). Receiver operating characteristic analysis revealed the threshold values of AR and LA ratio to be 1.18 and 1.50, respectively.
CONCLUSION
Age (≥60 yr), cerebral atherosclerosis, and aneurysms with a larger neck width and larger LA ratio are protective factors against bifurcation aneurysm rupture. An aneurysm with an irregular shape and an increased AR reflect the greater likelihood of a rupture.
Keyword
MeSH Terms
-
Adult
Age Factors
Aged
Aged, 80 and over
Aneurysm, Ruptured/*diagnostic imaging
Cerebral Angiography/*methods
*Computed Tomography Angiography
Developmental Disabilities
Diabetic Angiopathies/complications
Female
Humans
Hypertension/complications
Intracranial Aneurysm/*diagnostic imaging
Intracranial Arteriosclerosis/complications
Logistic Models
Male
Middle Aged
Middle Cerebral Artery/diagnostic imaging
Odds Ratio
Protective Factors
ROC Curve
Retrospective Studies
Risk Factors
Figure
-
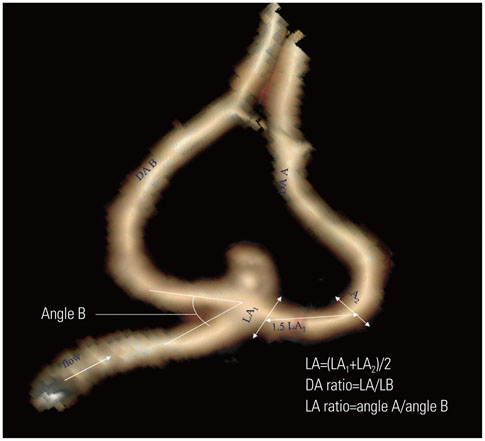
Fig. 1 The image of an aneurysm is classified as a classical neck type (Type C). The larger DA is defined as DA A, and the other DA is defined as DA B. LA mean diameter of the vessel measure at the LA1 and LA2, and the other vessel is measured as LB; the DA ratio is defined as LA/LB. The angle between the parent artery and DA A is defined as angle A, and the angle between the parent artery and DA B is defined as angle B; the LA ratio is defined as angle A/angle B. DA, daughter artery; LA ratio, lateral angle ratio; LA, diameter of DA A; LB, diameter of DA B.
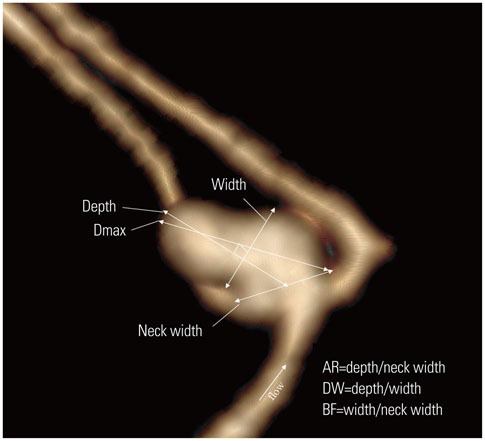
Fig. 2 The image of an aneurysm is classified as a deviated neck type (Type D). The image illustrates the method of dimension measurements: neck width, depth (the longest diameter between the neck and dome), width (the maximum distance vertical to height) and maximum size (Dmax, the largest measurement in terms of maximum dome diameter or width). Aspect ratio (AR) is calculated as depth divided by neck width, depth-to-width ratio (DW) is calculated as depth divided by width, and the bottleneck factor (BF) is calculated as width divided by neck width.
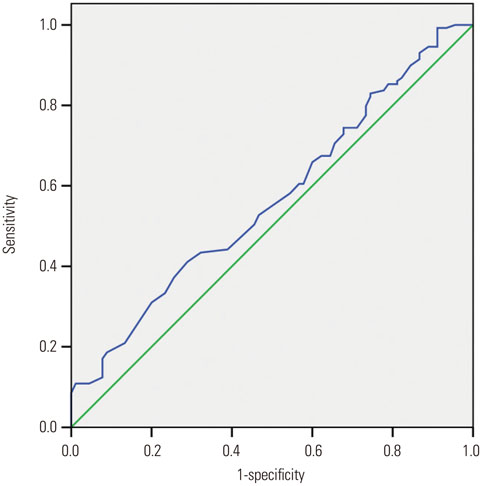
Fig. 3 The area under the receiver operating characteristic curve for the neck width is 0.566 (95% confidence interval, 0.490–0.642). The cut point for the neck width is 4.35 mm, the sensitivity is 67.4%, and the specificity is 40%.
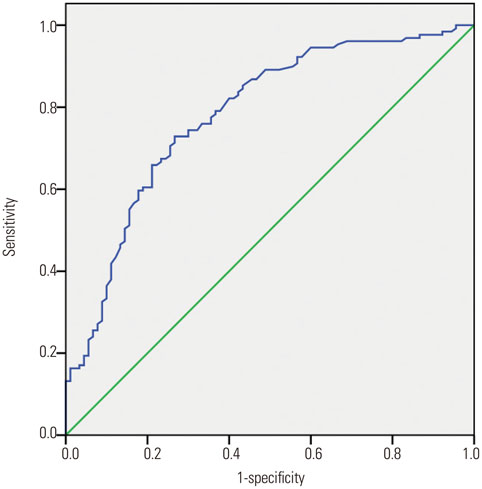
Fig. 4 The area under the receiver operating characteristic curve for the aspect ratio is 0.781 (95% confidence interval, 0.719–0.844). The cut point for the aspect ratio is 1.18, the sensitivity is 70.5%, and the specificity is 74.4%.
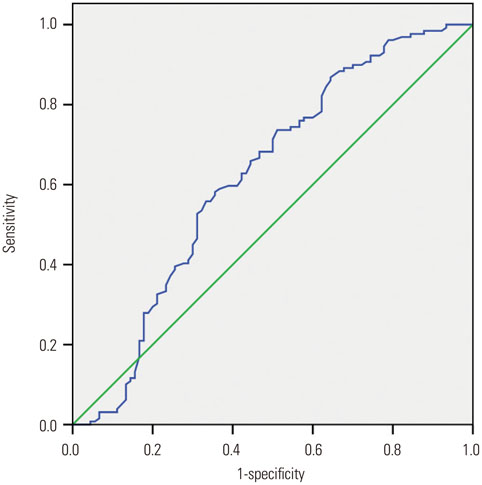
Fig. 5 The area under the receiver operating characteristic curve for the lateral angle ratio is 0.622 (95% confidence interval, 0.543–0.711). The cut point for the lateral angle ratio is 1.50, the sensitivity is 73.6%, and the specificity is 48.9%.
Cited by 1 articles
-
Comparison of Woven EndoBridge and stent-assisted coiling for treatment of acutely ruptured wide-neck bifurcation aneurysms: Single-center experience
Hossein Ghanaati, Aryoobarzan Rahmatian, Amir Torkaman, Mohammad Dashtkoohi, Mohammad Amin Dabbagh Ohadi
J Cerebrovasc Endovasc Neurosurg. 2025;27(1):33-39. doi: 10.7461/jcen.2024.E2024.11.002.
Reference
-
1. van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet. 2007; 369:306–318.
Article2. Ujiie H, Sato K, Onda H, Oikawa A, Kagawa M, Takakura K, et al. Clinical analysis of incidentally discovered unruptured aneurysms. Stroke. 1993; 24:1850–1856.
Article3. Jang EW, Kim YB, Chung J, Suh SH, Hong CK, Joo JY. Clinical risk factors affecting procedure-related major neurological complications in unruptured intracranial aneurysms. Yonsei Med J. 2015; 56:987–992.
Article4. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–110.
Article5. Baharoglu MI, Lauric A, Gao BL, Malek AM. Identification of a dichotomy in morphological predictors of rupture status between sidewall- and bifurcation-type intracranial aneurysms. J Neurosurg. 2012; 116:871–881.
Article6. Sadatomo T, Yuki K, Migita K, Taniguchi E, Kodama Y, Kurisu K. Morphological differences between ruptured and unruptured cases in middle cerebral artery aneurysms. Neurosurgery. 2008; 62:602–609.
Article7. Sadatomo T, Yuki K, Migita K, Taniguchi E, Kodama Y, Kurisu K. Evaluation of relation among aneurysmal neck, parent artery, and daughter arteries in middle cerebral artery aneurysms, by three-dimensional digital subtraction angiography. Neurosurg Rev. 2005; 28:196–200.
Article8. Sadatomo T, Yuki K, Migita K, Taniguchi E, Kodama Y, Kurisu K. The characteristics of the anterior communicating artery aneurysm complex by three-dimensional digital subtraction angiography. Neurosurg Rev. 2006; 29:201–207.
Article9. Rahman M, Ogilvy CS, Zipfel GJ, Derdeyn CP, Siddiqui AH, Bulsara KR, et al. Unruptured cerebral aneurysms do not shrink when they rupture: multicenter collaborative aneurysm study group. Neurosurgery. 2011; 68:155–160.
Article10. Lim YC, Kim CH, Kim YB, Joo JY, Shin YS, Chung J. Incidence and risk factors for rebleeding during cerebral angiography for ruptured intracranial aneurysms. Yonsei Med J. 2015; 56:403–409.
Article11. Ryu CW, Kwon OK, Koh JS, Kim EJ. Analysis of aneurysm rupture in relation to the geometric indices: aspect ratio, volume, and volume-to-neck ratio. Neuroradiology. 2011; 53:883–889.
Article12. You SH, Kong DS, Kim JS, Jeon P, Kim KH, Roh HK, et al. Characteristic features of unruptured intracranial aneurysms: predictive risk factors for aneurysm rupture. J Neurol Neurosurg Psychiatry. 2010; 81:479–484.
Article13. Aarhus M, Helland CA, Wester K. Differences in anatomical distribution, gender, and sidedness between ruptured and unruptured intracranial aneurysms in a defined patient population. Acta Neurochir (Wien). 2009; 151:1569–1574.
Article14. Inagawa T. Risk factors for the formation and rupture of intracranial saccular aneurysms in Shimane, Japan. World Neurosurg. 2010; 73:155–164.
Article15. Lall RR, Eddleman CS, Bendok BR, Batjer HH. Unruptured intracranial aneurysms and the assessment of rupture risk based on anatomical and morphological factors: sifting through the sands of data. Neurosurg Focus. 2009; 26:E2.
Article16. Unruptured intracranial aneurysms--risk of rupture and risks of surgical intervention.International Study of Unruptured Intracranial Aneurysms Investigators. N Engl J Med. 1998; 339:1725–1733.17. Bacigaluppi S, Piccinelli M, Antiga L, Veneziani A, Passerini T, Rampini P, et al. Factors affecting formation and rupture of intracranial saccular aneurysms. Neurosurg Rev. 2014; 37:1–14.
Article18. Hoh BL, Sistrom CL, Firment CS, Fautheree GL, Velat GJ, Whiting JH, et al. Bottleneck factor and height-width ratio: association with ruptured aneurysms in patients with multiple cerebral aneurysms. Neurosurgery. 2007; 61:716–722.19. Beck J, Rohde S, el Beltagy M, Zimmermann M, Berkefeld J, Seifert V, et al. Difference in configuration of ruptured and unruptured intracranial aneurysms determined by biplanar digital subtraction angiography. Acta Neurochir (Wien). 2003; 145:861–865.
Article20. Ujiie H, Tamano Y, Sasaki K, Hori T. Is the aspect ratio a reliable index for predicting the rupture of a saccular aneurysm? Neurosurgery. 2001; 48:495–502.
Article21. Nader-Sepahi A, Casimiro M, Sen J, Kitchen ND. Is aspect ratio a reliable predictor of intracranial aneurysm rupture? Neurosurgery. 2004; 54:1343–1347.
Article22. Dhar S, Tremmel M, Mocco J, Kim M, Yamamoto J, Siddiqui AH, et al. Morphology parameters for intracranial aneurysm rupture risk assessment. Neurosurgery. 2008; 63:185–196.
Article23. Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: probability of and risk factors for aneurysm rupture. J Neurosurg. 2008; 108:1052–1060.
Article24. Villablanca JP, Duckwiler GR, Jahan R, Tateshima S, Martin NA, Frazee J, et al. Natural history of asymptomatic unruptured cerebral aneurysms evaluated at CT angiography: growth and rupture incidence and correlation with epidemiologic risk factors. Radiology. 2013; 269:258–265.
Article25. Mehan WA Jr, Romero JM, Hirsch JA, Sabbag DJ, Gonzalez RG, Heit JJ, et al. Unruptured intracranial aneurysms conservatively followed with serial CT angiography: could morphology and growth predict rupture? J Neurointerv Surg. 2014; 6:761–766.
Article
