Korean J Gastroenterol.
2015 Aug;66(2):98-105. 10.4166/kjg.2015.66.2.98.
Comparison between Endoscopic Therapy and Medical Therapy in Peptic Ulcer Patients with Adherent Clot: A Multicenter Prospective Observational Cohort Study
- Affiliations
-
- 1Department of Internal Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea. jungjt@cu.ac.kr
- 2Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu, Korea.
- 3Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea.
- 4Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea.
- 5Department of Internal Medicine, Dongguk University School of Medicine, Gyeongju, Korea.
- 6Department of Internal Medicine, Gyeongsang National University Hospital, Jinju, Korea.
- 7Department of Internal Medicine, Soonchunhyang University Gumi Hospital, Gumi, Korea.
- KMID: 2373321
- DOI: http://doi.org/10.4166/kjg.2015.66.2.98
Abstract
- BACKGROUND/AIMS
The optimal management of bleeding peptic ulcer with adherent clot remains controversial. The purpose of this study was to compare clinical outcome between endoscopic therapy and medical therapy. We also evaluated the risk factors of rebleeding in Forrest type IIB peptic ulcer.
METHODS
Upper gastrointestinal (UGI) bleeding registry data from 8 hospitals in Korea between February 2011 and December 2013 were reviewed and categorized according to the Forrest classification. Patients with acute UGI bleeding from peptic ulcer with adherent clots were enrolled.
RESULTS
Among a total of 1,101 patients diagnosed with peptic ulcer bleeding, 126 bleedings (11.4%) were classified as Forrest type IIB. Of the 126 patients with adherent clots, 84 (66.7%) received endoscopic therapy and 42 (33.3%) were managed with medical therapy alone. The baseline characteristics of patients in two groups were similar except for higher Glasgow Blatchford Score and pre-endoscopic Rockall score in medical therapy group. Bleeding related mortality (1.2% vs. 10%; p=0.018) and all cause mortality (3.7% vs. 20.0%; p=0.005) were significantly lower in the endoscopic therapy group. However, there was no difference between endoscopic therapy and medical therapy regarding rebleeding (7.1% vs. 9.5%; p=0.641). In multivariate analysis, independent risk factors of rebleeding were previous medication with aspirin and/or NSAID (OR, 13.1; p=0.025).
CONCLUSIONS
In patients with Forrest type IIB peptic ulcer bleeding, endoscopic therapy was associated with a significant reduction in bleeding related mortality and all cause mortality compared with medical therapy alone. Important risk factor of rebleeding was use of aspirin and/or NSAID.
Keyword
MeSH Terms
-
Aged
Aged, 80 and over
Anti-Inflammatory Agents, Non-Steroidal/therapeutic use
Aspirin/therapeutic use
Cohort Studies
Female
*Hemostasis, Endoscopic
Humans
Male
Middle Aged
Multivariate Analysis
Peptic Ulcer/complications/diagnosis
Peptic Ulcer Hemorrhage/etiology/*therapy
Prospective Studies
Proton Pump Inhibitors/therapeutic use
Recurrence
Risk Factors
Treatment Outcome
Anti-Inflammatory Agents, Non-Steroidal
Aspirin
Proton Pump Inhibitors
Figure
-
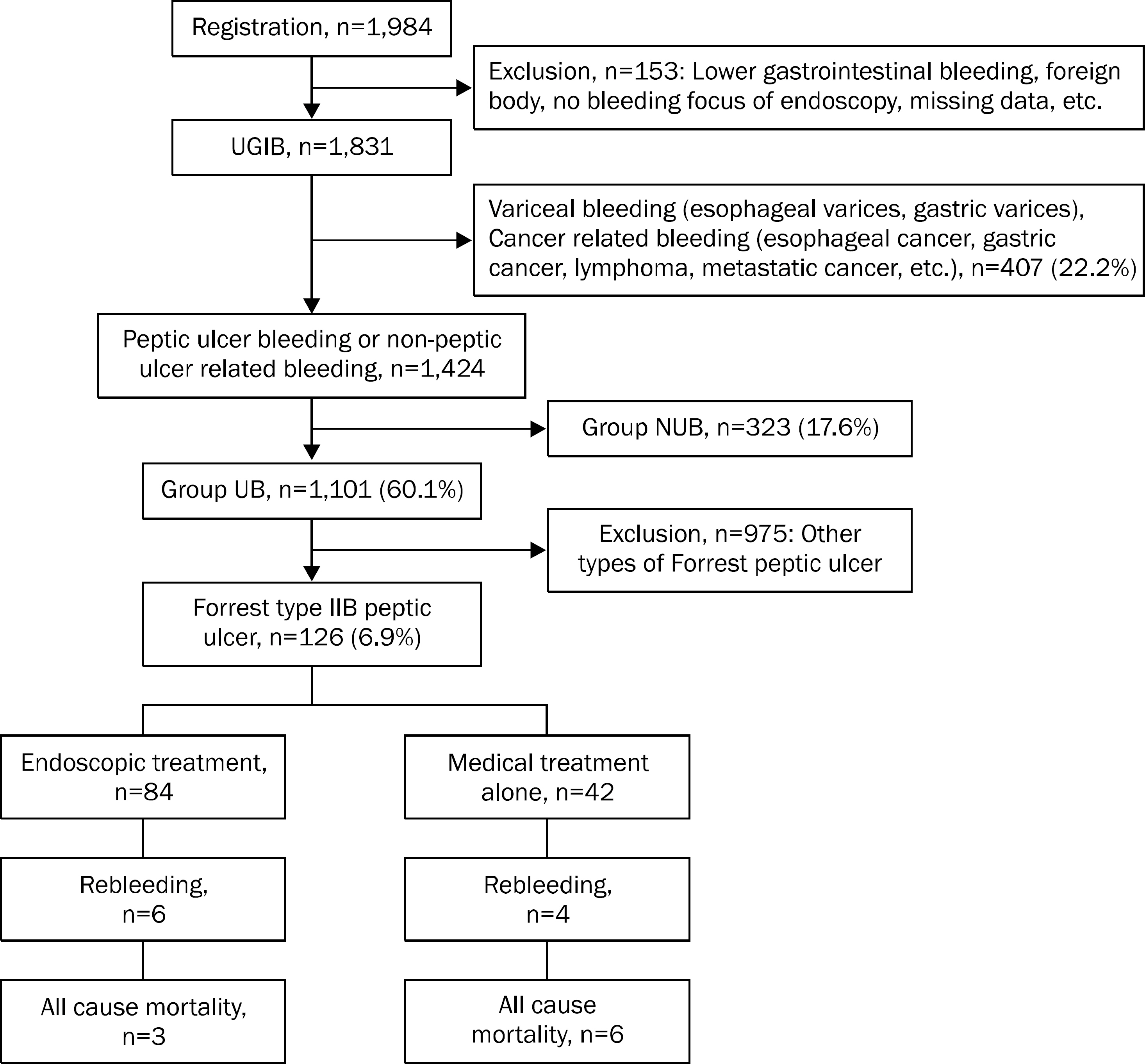
Fig. 1. Study flow showing the causes of upper gastrointestinal bleeding. The numbers in parentheses are the proportions of each group relating to patients with upper gastrointestinal bleeding (UGIB). GI, gastrointestinal; NUB, non-peptic ulcer related bleeding; UB, peptic ulcer bleeding.
Reference
-
References
1. van Leerdam ME, Vreeburg EM, Rauws EA, et al. Acute upper GI bleeding: did anything change? Time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003; 98:1494–1499.2. Hearnshaw SA, Logan RF, Lowe D, Travis SP, Murphy MF, Palmer KR. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut. 2011; 60:1327–1335.
Article3. Sung JJ, Kuipers EJ, El-Serag HB. Systematic review: the global incidence and prevalence of peptic ulcer disease. Aliment Pharmacol Ther. 2009; 29:938–946.
Article4. Kim JI, Kim SG, Kim N, et al. Korean College of Helicobacter and Upper Gastrointestinal Research. Changing prevalence of upper gastrointestinal disease in 28 893 Koreans from 1995 to 2005. Eur J Gastroenterol Hepatol. 2009; 21:787–793.5. Theocharis GJ, Thomopoulos KC, Sakellaropoulos G, Katsakoulis E, Nikolopoulou V. Changing trends in the epidemiology and clinical outcome of acute upper gastrointestinal bleeding in a defined geographical area in Greece. J Clin Gastroenterol. 2008; 42:128–133.
Article6. Hwang JH, Fisher DA, Ben-Menachem T, et al. Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in the management of acute non-variceal upper GI bleeding. Gastrointest Endosc. 2012; 75:1132–1138.
Article7. Enestvedt BK, Gralnek IM, Mattek N, Lieberman DA, Eisen G. An evaluation of endoscopic indications and findings related to non-variceal upper-GI hemorrhage in a large multicenter consortium. Gastrointest Endosc. 2008; 67:422–429.8. Proceedings of the Consensus Conference on Therapeutic Endoscopy in Bleeding Ulcers. March 6–8, 1989. Gastrointest Endosc. 1990; 36(5 Suppl):S1–S65.9. Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med. 1994; 331:717–727.
Article10. Laine L, Stein C, Sharma V. A prospective outcome study of patients with clot in an ulcer and the effect of irrigation. Gastrointest Endosc. 1996; 43:107–110.
Article11. Jensen DM, Kovacs TO, Jutabha R, et al. Randomized trial of medical or endoscopic therapy to prevent recurrent ulcer hemorrhage in patients with adherent clots. Gastroenterology. 2002; 123:407–413.
Article12. Bleau BL, Gostout CJ, Sherman KE, et al. Recurrent bleeding from peptic ulcer associated with adherent clot: a randomized study comparing endoscopic treatment with medical therapy. Gastrointest Endosc. 2002; 56:1–6.
Article13. Kahi CJ, Jensen DM, Sung JJ, et al. Endoscopic therapy versus medical therapy for bleeding peptic ulcer with adherent clot: a metaanalysis. Gastroenterology. 2005; 129:855–862.
Article14. Laine L. Systematic review of endoscopic therapy for ulcers with clots: can a metaanalysis be misleading? Gastroenterology. 2005; 129:2127. author reply 2127–8.
Article15. Laine L, McQuaid KR. Endoscopic therapy for bleeding ulcers: an evidence-based approach based on meta-analyses of randomized controlled trials. Clin Gastroenterol Hepatol. 2009; 7:33–47.
Article16. Jung HK, Son HY, Jung SA, et al. Comparison of oral omeprazole and endoscopic ethanol injection therapy for prevention of recurrent bleeding from peptic ulcers with nonbleeding visible vessels or fresh adherent clots. Am J Gastroenterol. 2002; 97:1736–1740.
Article17. Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet. 2000; 356:1318–1321.
Article18. Vreeburg EM, Terwee CB, Snel P, et al. Validation of the Rockall risk scoring system in upper gastrointestinal bleeding. Gut. 1999; 44:331–335.
Article19. Park JK, Jung YD, Seo YJ, et al. Risk factors for early rebleeding after initial endoscopic hemostasis in patients with bleeding peptic ulcers. Korean J Gastrointest Endosc. 2000; 21:898–908.20. Silverstein FE, Gilbert DA, Tedesco FJ, Buenger NK, Persing J. The national ASGE survey on upper gastrointestinal bleeding. II. Clinical prognostic factors. Gastrointest Endosc. 1981; 27:80–93.21. Rockall TA, Logan RF, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage. Gut. 1996; 38:316–321.
Article22. Ohmann C, Imhof M, Ruppert C, et al. Time-trends in the epidemiology of peptic ulcer bleeding. Scand J Gastroenterol. 2005; 40:914–920.
Article23. Gabriel SE, Jaakkimainen L, Bombardier C. Risk for serious gastrointestinal complications related to use of nonsteroidal anti-inflammatory drugs. A metaanalysis. Ann Intern Med. 1991; 115:787–796.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Oral Omeprazole Administration with Endoscopic Ethanol Injection Therapy for the Prevention of Recurrent Bleeding from Peptic Ulcers with Non-Bleeding Visible Vessels or Fresh Adherent Clots : A Prospective Randomized Trial
- Recent Developments in the Endoscopic Treatment of Patients with Peptic Ulcer Bleeding
- Comparison of Hemostatic Effects between a Combination Therapy Including Endoscopic Injection Therapy and Omeprazole and a Single Intravenous Omeprazole Therapy in Patients with Bleeding Peptic Ulcers
- Endoscopic treatment and pharmacologic therapy of peptic ulcer bleeding
- Hemostatic Effect of Endoscopic Injection with Hypertonic Saline Epinephrine for Peptic Ulcer Bleeding
