Diagnostic Value of Clinical T Staging Assessed by Endoscopy and Stomach Protocol Computed Tomography in Gastric Cancer: The Experience of a Low-Volume Institute
- Affiliations
-
- 1Department of Surgery, Jeju National University School of Medicine, Jeju, Korea. jeong445@jejunu.ac.kr
- 2Department of Radiology, Jeju National University School of Medicine, Jeju, Korea.
- 3Department of Gastroenterology, Jeju National University School of Medicine, Jeju, Korea.
- 4Department of Pathology, Jeju National University School of Medicine, Jeju, Korea.
Abstract
- PURPOSE
Clinical staging of gastric cancer appears to be important more and more for tailored therapy. This study aimed to verify the accuracy of clinical T staging in a low-volume institute.
MATERIALS AND METHODS
We retrospectively reviewed prospectively collected data of gastric cancer patients who underwent resection. A total of 268 patients of gastric cancer were enrolled from March 2004 to June 2012. These demographics, tumor characteristics, and clinical stages were analyzed for identification of diagnostic value of clinical T staging.
RESULTS
The predictive values for pT1 of endoscopy and computed tomography were 90.0% and 89.4%, respectively. In detail, the predictive values of endoscopy for pT1a, pT1b, and pT2 or more were 87%, 58.5%, and 90.6%, respectively. The predictive values of computed tomography for pT1a, pT1b, and pT2 or more were 68.8%, 73.9%, and 84.4%, respectively. The factors leading to underestimation of pT2 or more lesions by gastroscopy were the middle third location, the size greater than 2 cm, and younger age. Those for overestimation of pT1 lesion by computed tomography were male, age more than 70 years, elevated type, and size greater than 3 cm.
CONCLUSIONS
Diagnostic accuracy of early gastric cancer was 90%, which is comparable to those of high volume center. In patients with early gastric cancer, limited gastrectomy or minimal invasive surgery can be safely introduced at a low volume center also. However, the surgeon of low-volume institute should consider the accuracy of clinical staging before extending the indication of limited treatment.
MeSH Terms
Figure
-
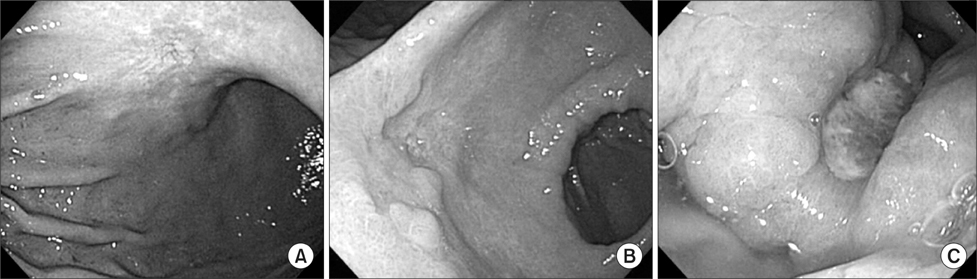
Fig. 1 Clinical T staging using gastroscopy. (A) A superficial spreading lesion with shallow and even depression corresponding to 'mucosa lesion'. (B) A deep ulceration with marked marginal elevation and abnormal converging folds corresponding to 'submucosa lesion'. (C) A ulcerative lesion surrounded by dam formation corresponding to 'advanced gastric cancer'.
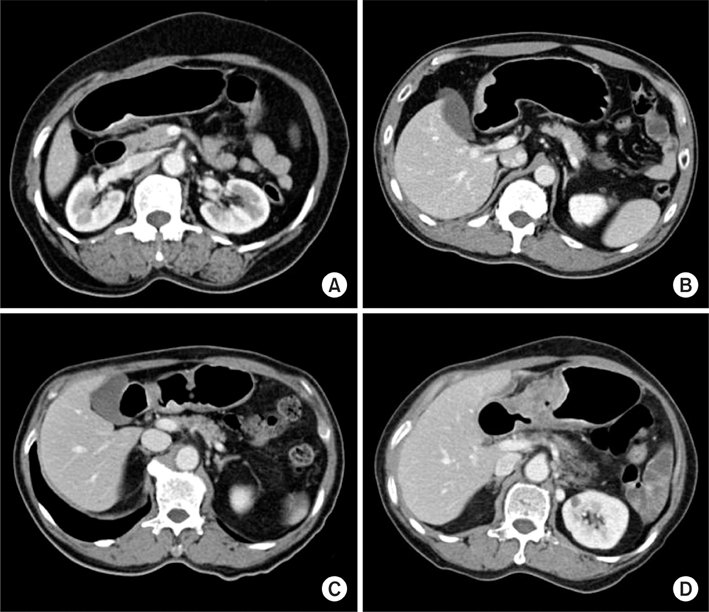
Fig. 2 Clinical T staging using stomach protocol computed tomography. (A) Enhancing mucosal thickening into middle layer with intact outer layers and a low-density-stripe layer corresponding to 'submucosal lesion'. (B) A enhancing lesion that reaches into outer layer with smooth outline corresponding to 'proper muscular lesion'. (C) Lesions without the discrimination between the enhancing gastric lesion and the outer layer with a few small linear stranding in the perigastric fat plane corresponding to 'subserosal lesion'. (D) Lesions with gastric wall thickening with spiculation and the preservation of fat plane between the gastric lesion and adjacent organ corresponding to 'serosal lesion'.
Reference
-
1. Kumano S, Murakami T, Kim T, Hori M, Iannaccone R, Nakata S, et al. T staging of gastric cancer: role of multi-detector row CT. Radiology. 2005. 237:961–966.
Article2. Cidón EU, Cuenca IJ. Gastric adenocarcinoma: is computed tomography (CT) useful in preoperative staging? Clin Med Oncol. 2009. 3:91–97.
Article3. Ohtani H, Tamamori Y, Noguchi K, Azuma T, Fujimoto S, Oba H, et al. A meta-analysis of randomized controlled trials that compared laparoscopy-assisted and open distal gastrectomy for early gastric cancer. J Gastrointest Surg. 2010. 14:958–964.
Article4. Kim AY, Kim HJ, Ha HK. Gastric cancer by multidetector row CT: preoperative staging. Abdom Imaging. 2005. 30:465–472.
Article5. Choi J, Kim SG, Im JP, Kim JS, Jung HC, Song IS. Endoscopic prediction of tumor invasion depth in early gastric cancer. Gastrointest Endosc. 2011. 73:917–927.
Article6. Park JM, Ahn CW, Yi X, Hur H, Lee KM, Cho YK, et al. Efficacy of endoscopic ultrasonography for prediction of tumor depth in gastric cancer. J Gastric Cancer. 2011. 11:109–115.
Article7. Ahn HS, Lee HJ, Yoo MW, Kim SG, Im JP, Kim SH, et al. Diagnostic accuracy of T and N stages with endoscopy, stomach protocol CT, and endoscopic ultrasonography in early gastric cancer. J Surg Oncol. 2009. 99:20–27.
Article8. Kim M, Park J, Kim SG, Choi S, Yoon S, Lee S. Feasibility of gastric cancer surgery at low volume hospitals. J Gastric Cancer. 2010. 10:234–240.
Article9. Kim JW, Shin SS, Heo SH, Choi YD, Lim HS, Park YK, et al. Diagnostic performance of 64-section CT using CT gastrography in preoperative T staging of gastric cancer according to 7th edition of AJCC cancer staging manual. Eur Radiol. 2012. 22:654–662.
Article10. Santiago JM, Sasako M, Osorio J. TNM-7th edition 2009 (UICC/AJCC) and Japanese Classification 2010 in Gastric Cancer. Towards simplicity and standardisation in the management of gastric cancer. Cir Esp. 2011. 89:275–281.
Article11. Dikken JL, van de Velde CJ, Gönen M, Verheij M, Brennan MF, Coit DG. The New American Joint Committee on Cancer/International Union Against Cancer staging system for adenocarcinoma of the stomach: increased complexity without clear improvement in predictive accuracy. Ann Surg Oncol. 2012. 19:2443–2451.
Article12. Bhandari S, Shim CS, Kim JH, Jung IS, Cho JY, Lee JS, et al. Usefulness of three-dimensional, multidetector row CT (virtual gastroscopy and multiplanar reconstruction) in the evaluation of gastric cancer: a comparison with conventional endoscopy, EUS, and histopathology. Gastrointest Endosc. 2004. 59:619–626.
Article13. Yanai H, Matsumoto Y, Harada T, Nishiaki M, Tokiyama H, Shigemitsu T, et al. Endoscopic ultrasonography and endoscopy for staging depth of invasion in early gastric cancer: a pilot study. Gastrointest Endosc. 1997. 46:212–216.
Article14. Yang SJ, Ahn EJ, Park SH, Kim JH, Park JM. The early experience of laparoscopy-assisted gastrectomy for gastric cancer at a low-volume center. J Gastric Cancer. 2010. 10:241–246.
Article15. Shin RM, Lee JH, Lee MS, Park DJ, Kim HH, Yang HK, et al. Analysis of diagnostic performance of CT and EUS for clinical TN staging of gastric cancer. J Korean Gastric Cancer Assoc. 2009. 9:177–185.
Article16. Lee JA, Park JH, Lee EJ, Kim SY, Kim Y, Lee SI. High-quality, low-cost gastrectomy care at high-volume hospitals: results from a population-based study in South Korea. Arch Surg. 2011. 146:930–936.
Article17. Choi J, Kim SG, Im JP, Kim JS, Jung HC, Song IS. Is endoscopic ultrasonography indispensable in patients with early gastric cancer prior to endoscopic resection? Surg Endosc. 2010. 24:3177–3185.
Article18. Choi J, Kim SG, Im JP, Kim JS, Jung HC, Song IS. Comparison of endoscopic ultrasonography and conventional endoscopy for prediction of depth of tumor invasion in early gastric cancer. Endoscopy. 2010. 42:705–713.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative N Staging of Gastric Cancer by Stomach Protocol Computed Tomography
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Spiral CT of the Gastric Adenocarcinoma
- Imaging Diagnosis of Gastric Cancer: CT Scan
- F18-fluorodeoxyglucose-positron emission tomography and computed tomography is not accurate in preoperative staging of gastric cancer
