Preoperative N Staging of Gastric Cancer by Stomach Protocol Computed Tomography
- Affiliations
-
- 1Department of Surgery, Jeju National University School of Medicine, Jeju, Korea. jeong445@jejunu.ac.kr
- 2Department of Radiology, Jeju National University School of Medicine, Jeju, Korea.
- 3Department of Pathology, Jeju National University School of Medicine, Jeju, Korea.
Abstract
- PURPOSE
Clinical stage of gastric cancer is currently assessed by computed tomography. Accurate clinical staging is important for the tailoring of therapy. This study evaluated the accuracy of clinical N staging using stomach protocol computed tomography.
MATERIALS AND METHODS
Between March 2004 and November 2012, 171 patients with gastric cancer underwent preoperative stomach protocol computed tomography (Jeju National University Hospital; Jeju, Korea). Their demographic and clinical characteristics were reviewed retrospectively. Two radiologists evaluated cN staging using axial and coronal computed tomography images, and cN stage was matched with pathologic results. The diagnostic accuracy of stomach protocol computed tomography for clinical N staging and clinical characteristics associated with diagnostic accuracy were evaluated.
RESULTS
The overall accuracy of stomach protocol computed tomography for cN staging was 63.2%. Computed tomography images of slice thickness 3.0 mm had a sensitivity of 60.0%; a specificity of 89.6%; an accuracy of 78.4%; and a positive predictive value of 78.0% in detecting lymph node metastases. Underestimation of cN stage was associated with larger tumor size (P<0.001), undifferentiated type (P=0.003), diffuse type (P=0.020), more advanced pathologic stage (P<0.001), and larger numbers of harvested and metastatic lymph nodes (P<0.001 each). Tumor differentiation was an independent factor affecting underestimation by computed tomography (P=0.045).
CONCLUSIONS
Computed tomography with a size criterion of 8 mm is highly specific but relatively insensitive in detecting nodal metastases. Physicians should keep in mind that computed tomography may not be an appropriate tool to detect nodal metastases for choosing appropriate treatment.
MeSH Terms
Figure
-
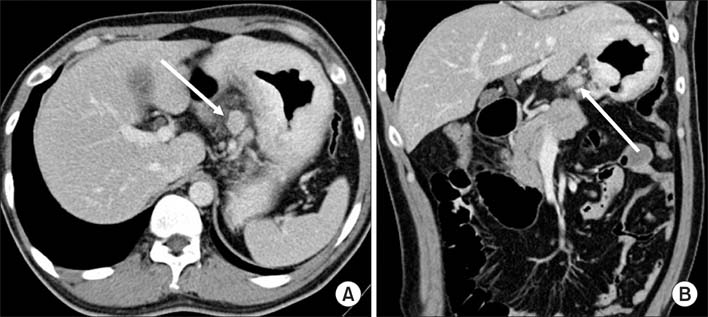
Fig. 1 Clinical N staging using stomach protocol computed tomography: A 15 mm sized lymph node (arrows) is seen along the left gastric artery (A, B). This was proven metastatic lymph node by pathological examination.
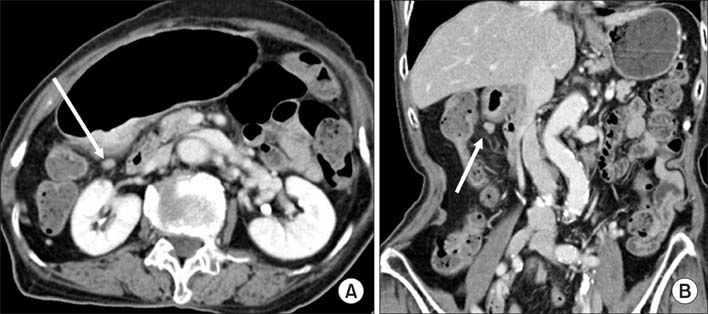
Fig. 2 Clinical N staging using stomach protocol computed tomography: Contrast enhanced computed tomography shows a small lymph node along the lesser curvature (arrows in A, B). The size of this lymph node was 8.3 mm in short diameter on axial image. However, it was no evidence of metastasis by pathological examination.
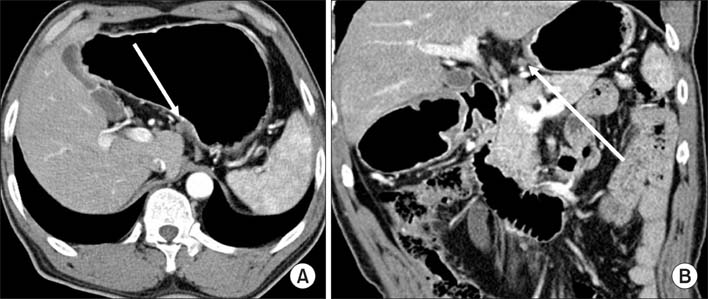
Fig. 3 Clinical N staging using stomach protocol computed tomography: Contrast-enhanced computed tomography shows a 5.3 mm sized lymph node in infrapyloric area (arrows in A, B). The computed tomography number of this lymph node was measured about 115 HU on the average. This was revealed metastatic lymph node by pathological examination.
Reference
-
1. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004; 54:8–29.
Article2. Jung KW, Park S, Kong HJ, Won YJ, Boo YK, Shin HR, et al. Cancer statistics in Korea: incidence, mortality and survival in 2006-2007. J Korean Med Sci. 2010; 25:1113–1121.
Article3. Kim YW, Yoon HM, Eom BW, Park JY. History of minimally invasive surgery for gastric cancer in Korea. J Gastric Cancer. 2012; 12:13–17.
Article4. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–123.
Article5. Park SR, Kim MJ, Ryu KW, Lee JH, Lee JS, Nam BH, et al. Prognostic value of preoperative clinical staging assessed by computed tomography in resectable gastric cancer patients: a viewpoint in the era of preoperative treatment. Ann Surg. 2010; 251:428–435.
Article6. Jeong JY, Kim MG, Ha TK, Kwon SJ. Prognostic factors on overall survival in lymph node negative gastric cancer patients who underwent curative resection. J Gastric Cancer. 2012; 12:210–216.
Article7. Son T, Hyung WJ, Lee JH, Kim YM, Kim HI, An JY, et al. Clinical implication of an insufficient number of examined lymph nodes after curative resection for gastric cancer. Cancer. 2012; 118:4687–4693.
Article8. Lee IJ, Lee JM, Kim SH, Shin CI, Lee JY, Kim SH, et al. Diagnostic performance of 64-channel multidetector CT in the evaluation of gastric cancer: differentiation of mucosal cancer (T1a) from submucosal involvement (T1b and T2). Radiology. 2010; 255:805–814.9. Hur J, Park MS, Lee JH, Lim JS, Yu JS, Hong YJ, et al. Diagnostic accuracy of multidetector row computed tomography in T- and N staging of gastric cancer with histopathologic correlation. J Comput Assist Tomogr. 2006; 30:372–377.10. Chen CY, Hsu JS, Wu DC, Kang WY, Hsieh JS, Jaw TS, et al. Gastric cancer: preoperative local staging with 3D multidetector row CT--correlation with surgical and histopathologic results. Radiology. 2007; 242:472–482.
Article11. Kim TH, Kim JJ, Kim SH, Kim BS, Song HJ, Na SY, et al. Diagnostic value of clinical T staging assessed by endoscopy and stomach protocol computed tomography in gastric cancer: the experience of a low-volume institute. J Gastric Cancer. 2012; 12:223–231.
Article12. Lee HH, Lim CH, Park JM, Cho YK, Song KY, Jeon HM, et al. Low accuracy of endoscopic ultrasonography for detailed T staging in gastric cancer. World J Surg Oncol. 2012; 10:190.
Article13. Ahn HS, Lee HJ, Yoo MW, Kim SG, Im JP, Kim SH, et al. Diagnostic accuracy of T and N stages with endoscopy, stomach protocol CT, and endoscopic ultrasonography in early gastric cancer. J Surg Oncol. 2009; 99:20–27.
Article14. Kang BC, Kim JH, Kim KW, Lee DY, Baek SY, Lee SW, et al. Value of the dynamic and delayed MR sequence with Gd-DTPA in the T-staging of stomach cancer: correlation with the histopathology. Abdom Imaging. 2000; 25:14–24.15. Yun M, Lim JS, Noh SH, Hyung WJ, Cheong JH, Bong JK, et al. Lymph node staging of gastric cancer using (18)F-FDG PET: a comparison study with CT. J Nucl Med. 2005; 46:1582–1588.16. Kwee RM, Kwee TC. Imaging in assessing lymph node status in gastric cancer. Gastric Cancer. 2009; 12:6–22.
Article17. Shinohara T, Ohyama S, Yamaguchi T, Muto T, Kohno A, Kato Y, et al. Clinical value of multidetector computed tomography in detecting lymph node metastasis of early gastric cancer. Eur J Surg Oncol. 2005; 31:743–748.
Article18. Stabile Ianora AA, Pedote P, Scardapane A, Memeo M, Rotondo A, Angelelli G. Preoperative staging of gastric carcinoma with multidetector spiral CT. Radiol Med. 2003; 106:467–480.
Article19. Morgagni P, Petrella E, Basile B, Mami A, Soro A, Gardini A, et al. Preoperative multidetector-row computed tomography scan staging for lymphatic gastric cancer spread. World J Surg Oncol. 2012; 10:197.
Article20. Park HS, Kim YJ, Ko SY, Yoo MW, Lee KY, Jung SI, et al. Benign regional lymph nodes in gastric cancer on multidetector row CT. Acta Radiol. 2012; 53:501–507.
Article21. Yan C, Zhu ZG, Yan M, Zhang H, Pan ZL, Chen J, et al. Value of multidetector-row computed tomography in the preoperative T and N staging of gastric carcinoma: a large-scale Chinese study. J Surg Oncol. 2009; 100:205–214.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- Imaging Diagnosis of Gastric Cancer: CT Scan
- Spiral CT of the Gastric Adenocarcinoma
- Diagnostic Importance of Preoperative Computed Tomography for Gastric Carcinoma
- Clinicopathologic Implication of New AJCC 8(th) Staging Classification in the Stomach Cancer
