Intraoperative Motor-Evoked Potential Disappearance versus Amplitude-Decrement Alarm Criteria During Cervical Spinal Surgery: A Long-Term Prognosis
- Affiliations
-
- 1Department of Neurology, Myung Diagnostic Radiology Clinic, Seoul, Korea.
- 2Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. chungc@snu.ac.kr
- 3Department of Neurology, Gachon University Gil Medical Center, Inchon, Korea.
- 4Department of Neurology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 5Department of Neurology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. sueh916@gmail.com
- KMID: 2364896
- DOI: http://doi.org/10.3988/jcn.2017.13.1.38
Abstract
- BACKGROUND AND PURPOSE
We studied the clinical significance of amplitude-reduction and disappearance alarm criteria for transcranial electric muscle motor-evoked potentials (MEPs) during cervical spinal surgery according to different lesion locations [intramedullary (IM) vs. nonintramedullary (NIM)] by evaluating the long-term postoperative motor status.
METHODS
In total, 723 patients were retrospectively dichotomized into the IM and NIM groups. Each limb was analyzed respectively. One hundred and sixteen limbs from 30 patients with IM tumors and 2,761 limbs from 693 patients without IM tumors were enrolled. Postoperative motor deficits were assessed up to 6 months after surgery.
RESULTS
At the end of surgery, 61 limbs (2.2%) in the NIM group and 14 limbs (12.1%) in the IM group showed MEP amplitudes that had decreased to below 50% of baseline, with 13 of the NIM limbs (21.3%) and 2 of the IM limbs (14.3%) showing MEP disappearance. Thirteen NIM limbs (0.5%) and 5 IM limbs (4.3%) showed postoperative motor deficits. The criterion for disappearance showed a lower sensitivity for the immediate motor deficit than did the criterion for amplitude decrement in both the IM and NIM groups. However, the disappearance criterion showed the same sensitivity as the 70%-decrement criterion in IM (100%) and NIM (83%) surgeries for the motor deficit at 6 months after surgery. Moreover, it has the highest specificity for the motor deficits among diverse alarm criteria, from 24 hours to 6 months after surgery, in both the IM and NIM groups.
CONCLUSIONS
The MEP disappearance alarm criterion had a high specificity in predicting the long-term prognosis after cervical spinal surgery. However, because it can have a low sensitivity in predicting an immediate postoperative deficit, combining different MEP alarm criteria according to the aim of specific instances of cervical spinal surgery is likely to be useful in practical intraoperative monitoring.
Keyword
MeSH Terms
Figure
-

Fig. 1 Case 1 showed the disappearance of the muscle motor-evoked potential (MEP) for the left abductor pollicis brevis (APB) and abductor hallucis. The patient showed postoperative motor deficits at the 24-hour and 6-month follow-up examinations. Case 2 showed MEP decrement on the left deltoid (18% remaining), biceps brachii (BB) (49% remaining), and APB (22% remaining). That patient showed a postoperative motor deficit after 24 hours but full recovery at the 6-month follow-up examination. Case 3 showed MEP decrement on the right BB (46% remaining). The patient showed postoperative motor deficits at the 24-hour and 6-month follow-up examinations. AH: abductor hallucis, DD: deltoid, MRC: Medical Research Council.
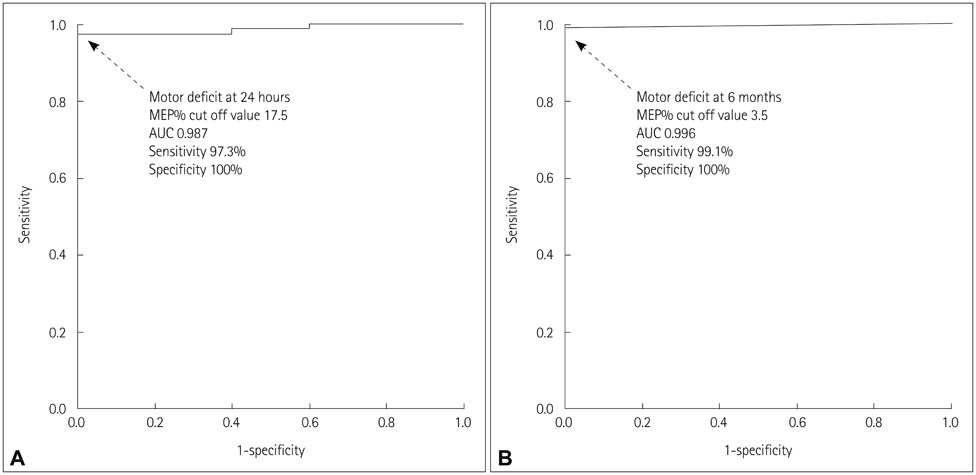
Fig. 2 Receiver operating characteristic curves of the intramedullary patients according to motor deficits at 24 hours (A) and 6 months (B). AUC: area under curve, MEP%: percentage of the final motor-evoked potential.

Fig. 3 ROC curves of the nonintramedullary (NIM) patients according to motor deficits at 24 hours (A) and 6 months (B). AUC: area under curve, MEP%: percentage of the final motor-evoked potential, ROC: receiver operating characteristic.

Fig. 4 Sensitivity (A, Left) and specificity (A, Right) of three different alarm criteria for cervical IM surgery according to the duration of postoperative motor deficits. The MEP disappearance alarm criterion showed the same sensitivity as other alarm criteria for 6-month postoperative motor deficits, and higher specificity than other alarm criteria for anytime postoperative motor deficits. Sensitivity (B, Left) and specificity (B, Right) of three different alarm criteria for cervical NIM surgery according to the duration of postoperative motor deficits. The MEP disappearance alarm criterion showed the same sensitivity as the 70%-decrement alarm criterion for 6-month postoperative motor deficits, and higher specificity than the other alarm criteria for anytime postoperative motor deficits. IM: intramedullary, MEP: motor-evoked potentials, NIM: nonintramedullary.
Reference
-
1. Nuwer MR, Emerson RG, Galloway G, Legatt AD, Lopez J, Minahan R, et al. Evidence-based guideline update: intraoperative spinal monitoring with somatosensory and transcranial electrical motor evoked potentials: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the American Clinical Neurophysiology Society. Neurology. 2012; 78:585–589.
Article2. Li F, Gorji R, Allott G, Modes K, Lunn R, Yang ZJ. The usefulness of intraoperative neurophysiological monitoring in cervical spine surgery: a retrospective analysis of 200 consecutive patients. J Neurosurg Anesthesiol. 2012; 24:185–190.
Article3. Ito Z, Imagama S, Sakai Y, Katayama Y, Wakao N, Ando K, et al. A new criterion for the alarm point for compound muscle action potentials. J Neurosurg Spine. 2012; 17:348–356.
Article4. Hyun SJ, Rhim SC. Combined motor and somatosensory evoked potential monitoring for intramedullary spinal cord tumor surgery: correlation of clinical and neurophysiological data in 17 consecutive procedures. Br J Neurosurg. 2009; 23:393–400.
Article5. Park P, Wang AC, Sangala JR, Kim SM, Hervey-Jumper S, Than KD, et al. Impact of multimodal intraoperative monitoring during correction of symptomatic cervical or cervicothoracic kyphosis. J Neurosurg Spine. 2011; 14:99–105.
Article6. Sakaki K, Kawabata S, Ukegawa D, Hirai T, Ishii S, Tomori M, et al. Warning thresholds on the basis of origin of amplitude changes in transcranial electrical motor-evoked potential monitoring for cervical compression myelopathy. Spine (Phila Pa 1976). 2012; 37:E913–E921.
Article7. Kobayashi S, Matsuyama Y, Shinomiya K, Kawabata S, Ando M, Kanchiku T, et al. A new alarm point of transcranial electrical stimulation motor evoked potentials for intraoperative spinal cord monitoring: a prospective multicenter study from the Spinal Cord Monitoring Working Group of the Japanese Society for Spine Surgery and Related Research. J Neurosurg Spine. 2014; 20:102–107.
Article8. Kim DH, Zaremski J, Kwon B, Jenis L, Woodard E, Bode R, et al. Risk factors for false positive transcranial motor evoked potential monitoring alerts during surgical treatment of cervical myelopathy. Spine (Phila Pa 1976). 2007; 32:3041–3046.
Article9. Sala F, Palandri G, Basso E, Lanteri P, Deletis V, Faccioli F, et al. Motor evoked potential monitoring improves outcome after surgery for intramedullary spinal cord tumors: a historical control study. Neurosurgery. 2006; 58:1129–1143. discussion 1129-1143.
Article10. Macdonald DB, Al Zayed Z, Al Saddigi A. Four-limb muscle motor evoked potential and optimized somatosensory evoked potential monitoring with decussation assessment: results in 206 thoracolumbar spine surgeries. Eur Spine J. 2007; 16:Suppl 2. S171–S187.
Article11. Kim SM, Yang H, Park SB, Han SG, Park KW, Yoon SH, et al. Pattern-specific changes and discordant prognostic values of individual leg-muscle motor evoked potentials during spinal surgery. Clin Neurophysiol. 2012; 123:1465–1470.
Article12. Burke D, Hicks R, Stephen J, Woodforth I, Crawford M. Trial-to-trial variability of corticospinal volleys in human subjects. Electroencephalogr Clin Neurophysiol. 1995; 97:231–237.
Article13. Macdonald DB, Skinner S, Shils J, Yingling C. American Society of Neurophysiological Monitoring. Intraoperative motor evoked potential monitoring - a position statement by the American Society of Neurophysiological Monitoring. Clin Neurophysiol. 2013; 124:2291–2316.
Article14. Calancie B, Molano MR. Alarm criteria for motor-evoked potentials: what's wrong with the “presence-or-absence” approach? Spine (Phila Pa 1976). 2008; 33:406–414.15. Quraishi NA, Lewis SJ, Kelleher MO, Sarjeant R, Rampersaud YR, Fehlings MG. Intraoperative multimodality monitoring in adult spinal deformity: analysis of a prospective series of one hundred two cases with independent evaluation. Spine (Phila Pa 1976). 2009; 34:1504–1512.16. Kleyweg RP, van der Meché FG, Schmitz PI. Interobserver agreement in the assessment of muscle strength and functional abilities in Guillain-Barré syndrome. Muscle Nerve. 1991; 14:1103–1109.
Article17. Sundaresan N, Digiacinto GV, Hughes JE, Cafferty M, Vallejo A. Treatment of neoplastic spinal cord compression: results of a prospective study. Neurosurgery. 1991; 29:645–650.
Article18. Benesch M, Weber-Mzell D, Gerber NU, von Hoff K, Deinlein F, Krauss J, et al. Ependymoma of the spinal cord in children and adolescents: a retrospective series from the HIT database. J Neurosurg Pediatr. 2010; 6:137–144.
Article19. Kiers L, Cros D, Chiappa KH, Fang J. Variability of motor potentials evoked by transcranial magnetic stimulation. Electroencephalogr Clin Neurophysiol. 1993; 89:415–423.
Article20. Sakaura H, Hosono N, Mukai Y, Ishii T, Yoshikawa H. C5 palsy after decompression surgery for cervical myelopathy: review of the literature. Spine (Phila Pa 1976). 2003; 28:2447–2451.21. Bhalodia VM, Schwartz DM, Sestokas AK, Bloomgarden G, Arkins T, Tomak P, et al. Efficacy of intraoperative monitoring of transcranial electrical stimulation-induced motor evoked potentials and spontaneous electromyography activity to identify acute-versus delayed-onset C-5 nerve root palsy during cervical spine surgery: clinical article. J Neurosurg Spine. 2013; 19:395–402.
Article22. Fujiwara Y, Manabe H, Izumi B, Tanaka H, Kawai K, Tanaka N. The efficacy of intraoperative neurophysiological monitoring using transcranial electrically stimulated muscle-evoked potentials (TcE-MsEPs) for predicting postoperative segmental upper extremity motor paresis after cervical laminoplasty. Clin Spine Surg. 2016; 29:E188–E195.
Article23. Tanaka N, Nakanishi K, Fujiwara Y, Kamei N, Ochi M. Postoperative segmental C5 palsy after cervical laminoplasty may occur without intraoperative nerve injury: a prospective study with transcranial electric motor-evoked potentials. Spine (Phila Pa 1976). 2006; 31:3013–3017.
Article24. Kothbauer KF, Deletis V, Epstein FJ. Motor-evoked potential monitoring for intramedullary spinal cord tumor surgery: correlation of clinical and neurophysiological data in a series of 100 consecutive procedures. Neurosurg Focus. 1998; 4:e1.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Motor Evoked Potential Improvement in Cervical Spondylotic Myelopathy: Comparison of Cortical Stimulation Parameters
- Facilitation of Magnetic Evoked Potential by Thinking of Motion
- Intraoperative Monitoring of Hypoglossal Nerve Using Hypoglossal Motor Evoked Potential in Infratentorial Tumor Surgery: A Report of Two Cases
- Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
