J Korean Ophthalmol Soc.
2013 Sep;54(9):1386-1394.
Relationship Between Nocturnal Dip, Carotid Artery Blood Flow, Brain Ischemic Change in Open Angle Glaucoma
- Affiliations
-
- 1Department of Ophthalmology, Dong-A University Medical Center, Dong-A University College of Medicine, Busan, Korea. shrho@donga.ac.kr
Abstract
- PURPOSE
To investigate the effect of nocturnal dip, carotid artery blood flow, and brain ischemic change on the progression of glaucomatous visual field defect in open-angle glaucoma (OAG) when IOP is less than the target pressure.
METHODS
We classified OAG patients (74 patients, 148 eyes) who maintained IOP less than the target pressure as normal tension glaucoma (NTG; 52 patients, 104 eyes) or primary OAG (POAG; 22 patients, 44 eyes). Additionally, we performed 24-hr ambulatory blood pressure monitoring (24-hr ABPM), carotid artery color Doppler U/S (CAD), brain MRI, and visual field (V/F) tests on the patients. Nocturnal dips less than 10% were classified as non-dippers, and dips greater than 10% as dippers. The relationships among nocturnal dip, carotid artery blood flow, brain ischemic change, and progression of glaucomatous V/F defect were examined.
RESULTS
In the case of dippers, glaucomatous V/F defects were aggravated, with a relative risk of approximately 1.74 (NTG) and 2.91 (POAG) times that of non-dippers. In NTG, decreased carotid artery blood flow and brain ischemic change furthered glaucomatous V/F defects, with a relative risk of approximately 2.40 and 2.54 times that of normal carotid artery blood flow and brain MRI findings, respectively. However, in POAG, decreased carotid artery blood flow and brain ischemic change were not influenced by the progression of glaucomatous V/F defects.
CONCLUSIONS
In dippers, decreased carotid artery blood flow and brain ischemic change caused a progression of glaucomatous V/F defects in NTG and POAG patients. Thus, performing 24-hr ABPM, CAD, and brain MRI should be helpful for glaucoma patients with progression of glaucomatous V/F defects even when the IOP is less than the target pressure. In addition, this analysis provides useful information regarding glaucoma diagnosis and treatment.
Keyword
MeSH Terms
Figure
-

Figure 1. Abnormal findings of CAD. (A) Increased intima-media thickness in left common carotid artery (white arrow). (B) Multiple atheromas in left internal carotid artery (white arrows).
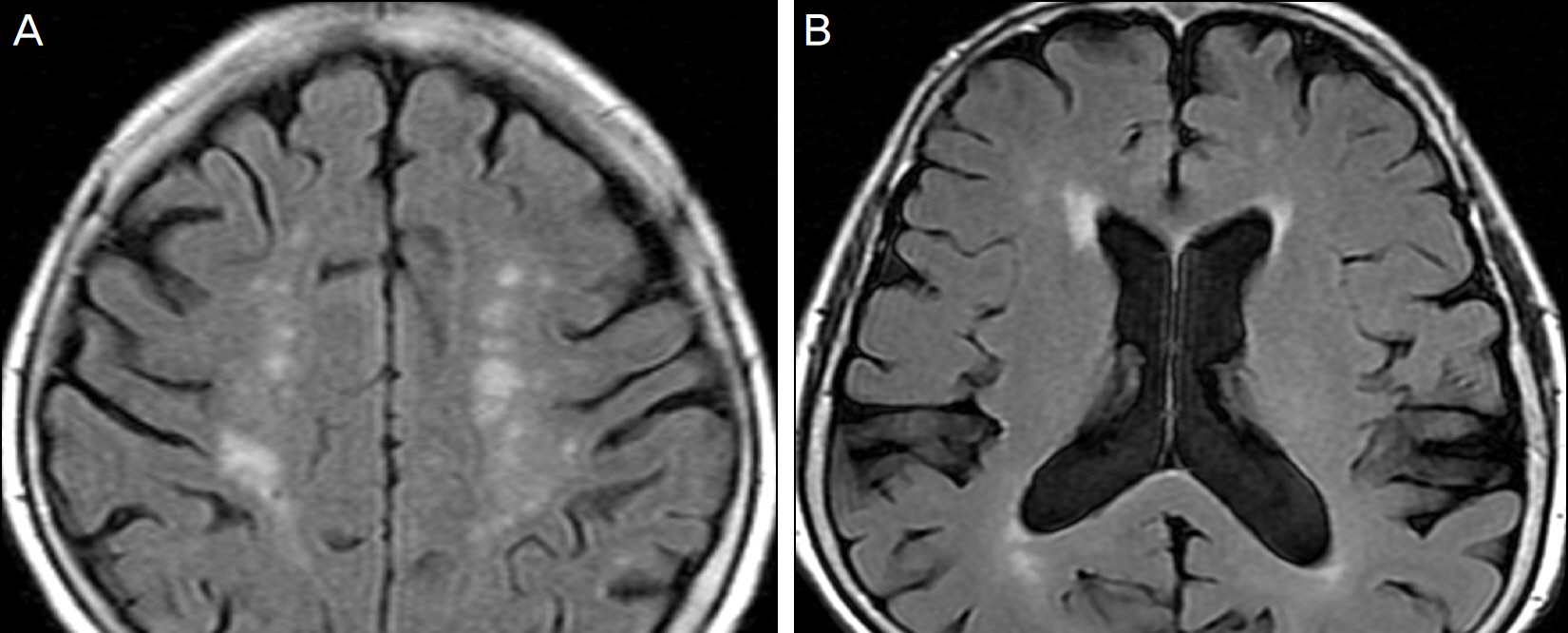
Figure 2. Abnormal findings of brain MRI. (A) Chronic ischemic change deep white matter, basal ganglia. (B) Brain atrophy. widening of the sulci, thinning of the corpus callosum, enlargement of the lateral ventricles.
Reference
-
References
1. Van Buskirk EM, Cioffi GA. Glaucomatous optic neuropathy. Am J Ophthalmol. 1992; 113:447–52.
Article2. Armaly MF. Ocular pressure and visual fields. A ten-year fol-low-up study. Arch Ophthalmol. 1969; 81:25–40.3. Levens RZ. Low tension glaucoma: a critical review and new material. Surv Ophthalmol. 1980; 24:621–64.4. Perkins ES. The Bedford glaucoma survey. I. Long-term follow-up of borderline cases. Br J Ophthalmol. 1973; 57:179–85.
Article5. Hayreh SS. Progress in the understanding of the vascular etiology of glaucoma. Curr Opin Ophthalmol. 1994; 5:26–35.
Article6. Cartwright MJ, Anderson DR. Correlation of asymmetric damage with asymmetric intraocular pressure in normal-tension glaucoma. Arch Ophthalmol. 1988; 106:898–900.7. Araie M, Sekine M, Suzuki Y, Koseki N. Factors contributing to the progression of visual field damage in eyes with normal tension glaucoma. Ophthalmology. 1994; 101:1440–4.8. Ishida K, Yamamoto T, Sugiyama K, Kitazawa Y. Disk hemor-rhage is a significantly negative prognostic factor in nor-mal-tension glaucoma. Am J Ophthalmol. 2000; 129:707–14.
Article9. Drance S, Anderson DR, Schulzer M. Risk factors for progression of visual field abnormalities in normal tension glaucoma. Am J Ophthalmol. 2001; 131:699–708.10. Zeimer RC, Wilensky JT, Gieser DK, Viana MA. Association be-tween intraocular pressure peaks and progression of visual fieldloss. Ophthalmology. 1991; 98:64–9.11. Brubaker RF. Delayed functional loss in glaucoma. LII Edward Jackson Memorial Lecture. Am J Ophthalmol. 1996; 121:473–83.
Article12. Hayreh SS. The blood supply of the optic nerve head and the evalu-ation of it: myth and reality. Prog Retin Eye Res. 2001; 20:563–93.13. Gherghel D, Orgül S, Gugleta K. . Relationship between ocular perfusion pressure and retrobulbar blood flow in patients with glaucoma with progressive damage. Am J Ophthalmol. 2000; 130:597–605.
Article14. Sehi M, Flanagan JG, Zeng L. . Relative change in diurnal mean ocular perfusion pressure: a risk factor for the diagnosis of primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 2005; 46:561–7.
Article15. Hayreh SS. Duke-elder Lecture. Systemic arterial blood pressure and the eye. Eye (Lond). 1996; 10((Pt 1)):5–28.16. Hayreh SS, Zimmerman MB, Podhajsky P, Alward WL. Nocturnal arterial hypotension and its role in optic nerve head and ocular is-chemic disorders. Am J Ophthalmol. 1994; 117:603–24.
Article17. Béchetoille A, Bresson-Dumont H. Diurnal and nocturnal blood pressure drops in patients with focal ischemic glaucoma. Graefes Arch Clin Exp Ophthalmol. 1994; 232:675–9.18. Seo HR, Ryu WY, Rho SH. Corrlelation between nocturnal dip and progression of glaucoma. J Korean Ophthalmol Soc. 2010; 51:1471–8.19. Baxter GM, Williamson TH. Color Doppler imaging of the eye: normal ranges, reproducibility, and observer variation. J Ultrasound Med. 1995; 14:91–6.
Article20. Niwa Y, Yamamoto T, Kawakami H. . Reproducibility of color Doppler imaging for orbital arteries in Japanese patients with nor-mal-tension glaucoma. Jpn J Ophthalmol. 1998; 42:389–92.
Article21. Birinci H, Danaci M, Oge I, Erkan ND. Ocular blood flow in healthy and primary open-angle glaucomatous eyes. Ophthalmologica. 2002; 216:434–7.
Article22. Galassi F, Nuzzaci G, Sodi A. . Color Doppler imaging in eval-uation of optic nerve blood supply in normal and glaucomatous subjects. Int Ophthalmol. 1992; 16:273–6.
Article23. Nicolela MT, Walman BE, Buckley AR, Drance SM. Ocular hyper-tension and primary open-angle glaucoma: a comparative study of their retrobulbar blood flow velocity. J Glaucoma. 1996; 5:308–10.24. Rankin SJ, Walman BE, Buckley AR, Drance SM. Color Doppler imaging and spectral analysis of the optic nerve vasculature in glaucoma. Am J Ophthalmol. 1995; 119:685–93.
Article25. Schumann J, Orgül S, Gugleta K. . Interocular difference in progression of glaucoma correlates with interocular differences in retrobulbar circulation. Am J Ophthalmol. 2000; 129:728–33.
Article26. Arsava EM. The role of MRI as a prognostic tool in ischemic stroke. J Neurochem. 2012; 123(Suppl 2):22–8.
Article27. Taha MM, Maeda M, Sakaida H. . Cerebral ischemic lesions detected with diffusion-weighted magnetic resonance imaging af-ter carotid artery stenting: Comparison of several anti-embolic pro-tection devices. Neurol Med Chir (Tokyo). 2009; 49:386–93.
Article28. Kim SJ, Roh HG, Jeon P. . Cerebral ischemia detected with dif-fusion-weighted MR imaging after protected carotid artery stenting: comparison of distal balloon and filter device. Korean J Radiol. 2007; 8:276–85.
Article29. Roher AE, Debbins JP. . Cerebral blood flow in Alzheimer's disease. Vasc Health Risk Manag. 2012; 8:599–611.30. Ong K, Farinelli A, Billson F. . Comparative study of brain magnetic resonance imaging findings in patients with low-tension glaucoma and control subjects. Ophthalmology. 1995; 102:1632–8.
Article31. Leung DY, Tham CC, Li FC. . Silent cerebral infarct and visual field progression in newly diagnosed normal-tension glaucoma: a cohort study. Ophthalmology. 2009; 116:1250–6.32. Collaborative Normal-Tension Glaucoma Study Group. The effectiveness of intraocular pressure reduction in the treatment of nor-mal-tension glaucoma. Am J Ophthalmol. 1998; 126:498–505.33. Advanced Glaucoma Intervention Study. 2. Visual field test scoring and reliability. Ophthalmology. 1994; 101:1445–55.34. Kim J, Dally LG, Ederer F. . The Advanced Glaucoma Intervention Study (AGIS): 14. Distinguishing progression of glaucoma from visu-al field fluctuations. Ophthalmology. 2004; 111:2109–16.35. Plange N, Kaup M, Daneljan L. . 24-h blood pressure monitoring in normal tension glaucoma: night-time blood pressure variability. J Hum Hypertens. 2006; 20:137–42.
Article36. Graham SL, Drance SM, Wijsman K. . Ambulatory blood pres-sure monitoring in glaucoma. The nocturnal dip. Ophthalmology. 1995; 102:61–9.37. Hirotsu C, Ohta E, Hirose N, Shimizu K. Profile analysis of 24-hours measurements of blood pressure. Biometrics. 2003; 59:907–15.
Article38. Choi J, Jeong J, Cho H, Kook MS. Effect of nocturnal blood pres-sure reduction on circadian fluctuation of mean ocular perfusion pressure: a risk factor for normal tension glaucoma. Invest Ophthalmol Vis Sci. 2006; 47:831–6.
Article39. Collignon N, Dewe W, Guillaume S, Collignon-Brach J. Ambulatory blood pressure monitoring in glaucoma patients. The nocturnal systolic dip and its relationship with disease progression. Int Ophthalmol. 1998; 22:19–25.40. Harris A, Rechtman E, Siesky B. . The role of optic nerve blood flow in the pathogenesis of glaucoma. Ophthalmol Clin North Am. 2005; 18:345–53, v.
Article41. Akarsu C, Bilgili MY. Color Doppler imaging in ocular hyper-tension and open-angle glaucoma. Grafes Arch Clin Exp Ophthalmol. 2004; 242:125–9.
Article42. Galassi F, Giambene B, Menchini U. Ocular perfusion pressure and retrobulbar haemodynamics in pseudoexfoliation glaucoma. Grafes Arch Clin Exp Ophthalmol. 2008; 246:411–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship among Water-Shed Zone, Nocturnal Dip and Visual Field Progression in Open Angle Glaucoma
- 24-hour Ambulatory Blood Pressure in Normal Tension Glaucoma: Associations with Retinal Vessel Diameter and Visual Field Defect Progression
- The Measurement of Ocular Blood Flow Velocity using Doppler Ultrasound in Normal Tension Glaucoma Patients
- A Case of Ocular Ischemic Syndrome Associated with Multiple Branch Retinal Artery Occlusion and Neovascular Glaucoma
- Difference in 24-Hour Ambulatory Blood Pressure in Normal Tension Glaucoma and Primary Open-Angle Glaucoma
