J Korean Orthop Assoc.
2011 Dec;46(6):523-527.
Traumatic Atlantoaxial Unifacetal Joint Dislocation Associated with Fractures of Ipsilateral C2 Body and Contralateral Pars
- Affiliations
-
- 1Department of Orthopedic Surgery, Graduate School of Medicine, Kyungpook National University, Daegu, Korea. wkmin@knu.ac.kr
Abstract
- The traumatic C1-C2 unifacetal joint dislocation associated with oblique fractures of the C2 body and arch is a rare injury that can be effectively treated with gentle closed reduction under fluoroscopic guidance followed by halo vest immobilization. To our knowledge, however, there are only a few reported cases of this injury. Recognition of associated conditions including vertebral artery compromise, concomitant cervical spine fractures, and life-threatening injuries is paramount to the successful treatment of these patients. A 29-year-old patient, who presented a unifacetal dislocation at C1-C2 with associated oblique fractures of the C2 body and arch, is reported. Closed reduction with Gardner-Wells tong and halo vest application was performed. After 3 months of application of halo vest, the fractures of C2 body and arch had the complete union and the C1-2 dislocation had the good reduction. He had no pain and discomfort in his neck for about 2 years after halo vest removal.
Figure
-

Figure 1 The open-mouth odontoid radiograph revealed slight rotation of C1 lateral mass.

Figure 2 The radiograph of the lateral cervical spine showed a facture of C2 pars interarticularis. But there was no translation or angulation of C1-C2 and C2-C3.
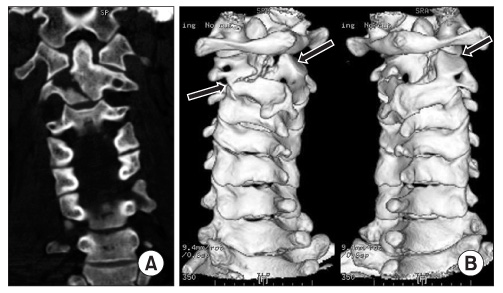
Figure 3 (A) The coronal view of computed tomography (CT) show the oblique body fracture of axis. (B) The three-dimensional CT scan demonstrated an atlantoaxial unifacetal dislocation and pars interarticulairs fracture of axis.

Figure 4 The plain lateral radiograph and the open-mouth odontoid radiograph showed the complete union of C2 fractures (body and pars interarticularis).
Reference
-
1. Schneider RC, Livingston KE, Cave AJ, Hamilton G. "Hangman's Fracture" of the cervical spine. J Neurosurg. 1965. 22:141–154.
Article2. Spoor AB, Diekerhof CH, Bonnet M, Oner FC. Traumatic complex dislocation of the atlanto-axial joint with odontoid and C2 superior articular facet fracture. Spine (Phila Pa 1976). 2008. 33:E708–E711.
Article3. Miyamoto H, Doita M, Nishida K, et al. Traumatic anterior atlantoaxial subluxation occurring in a professional rugby athlete: case report and review of literature related to atlantoaxial injuries in sports activities. Spine (Phila Pa 1976). 2004. 29:E61–E64.4. Francis WR, Fielding JW, Hawkins RJ, Pepin J, Hensinger R. Traumatic spondylolisthesis of the axis. J Bone Joint Surg Br. 1981. 63:313–318.
Article5. Singh VK, Singh PK, Balakrishnan SK, Leitao J. Traumatic bilateral atlantoaxial rotatory subluxation mimicking as torticollis in an adult female. J Clin Neurosci. 2009. 16:721–722.
Article6. Subach BR, McLaughlin MR, Albright AL, Pollack IF. Current management of pediatric atlantoaxial rotatory subluxation. Spine (Phila Pa 1976). 1998. 23:2174–2179.
Article7. Effendi B, Roy D, Cornish B, Dussault RG, Laurin CA. Fractures of the ring of the axis. A classification based on the analysis of 131 cases. J Bone Joint Surg Br. 1981. 63:319–327.
Article8. Levine AM, Edwards CC. The management of traumatic spondylolisthesis of the axis. J Bone Joint Surg Am. 1985. 67:217–226.
Article9. Goldberg W, Mueller C, Panacek E, Tigges S, Hoffman JR, Mower WR. NEXUS Group. Distribution and patterns of blunt traumatic cervical spine injury. Ann Emerg Med. 2001. 38:17–21.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Post-traumatic Atlantoaxial Rotatory Dislocation in an Adult Treated by Open Reduction and C1-C2 Transpedicular Screw Fixation
- A Traumatic Anterior Hip Dislocation Associated Ipsilateral Femoral Shaft Segmental Fracture : Case Report
- Hip Fracture-dislocation with Sciatic Nerve Palsy and Ipsilateral Femoral Shaft Open Fracture: A Case Report
- Posterior Hip Dislocation with Ipsilateral Fractures of the Femoral Head and Intertrochanter: A Case Report
- Treatment of Traumatic Sternoclavicular Joint Anterior Dislocation with a Sternal Fracture
