Tuberc Respir Dis.
2013 Jul;75(1):28-31.
Mycobacterium intracellulare Pulmonary Disease with Endobronchial Caseation in a Patient Treated with Methotrexate
- Affiliations
-
- 1Department of Internal Medicine, Gachon University Gil Hospital, Gachon University Medicine and Science, Incheon, Korea. allergy21@hotmail.com
- 2Department of Pathology, Ewha Womans University School of Medicine, Seoul, Korea. americandoc@hanmail.net
Abstract
- Methotrexate (MTX) has been established as a standard disease-modifying anti-rheumatic drug. If adequate disease control is achieved for a reasonable period of time, tapering the MTX dosage is recommended because the chronic use of MTX can result in opportunistic infection. We present here a case of a woman with rheumatoid arthritis taking MTX, and the woman developed actively caseating endobronchial Mycobacterium intracellulare disease with pulmonary infiltrations. After discontinuing the MTX, the patient was able to tolerate 18 months of antimycobacterial treatment without flare ups of rheumatoid arthritis, and she completely recovered from nontuberculous mycobacterial respiratory disease.
Keyword
MeSH Terms
Figure
-
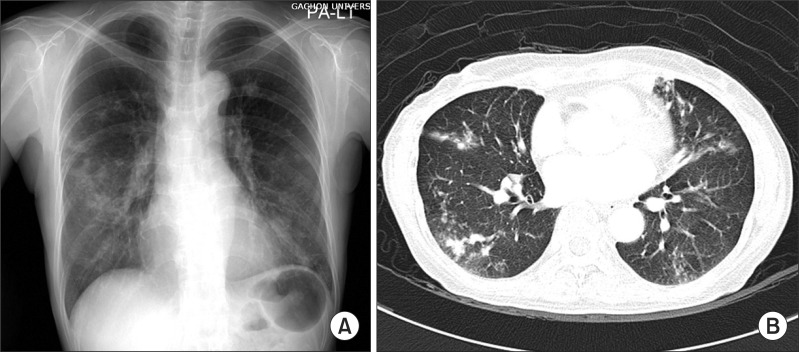
Figure 1 Plain radiography (A) and computed tomography (B) of the chest of a 58-year-old woman who was infected with Mycobacterium intracellulare showed multifocal nodular consolidation and ill-defined nodules in both lungs, and this was all more prominent in the mid-lung field of the right lung, without evidence of mediastinal lymphadenopathy.
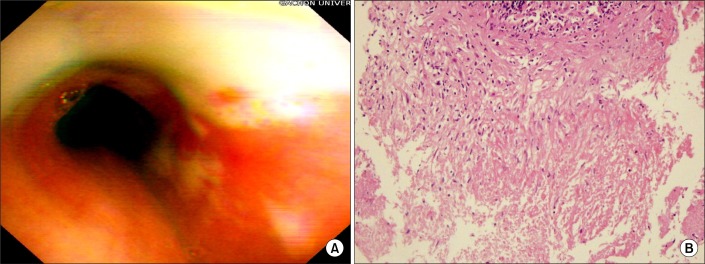
Figure 2 Bronchoscopic photograph of the left main (A) revealed diffuse actively caseating endobronchilal lesions. The bronchial biopsy specimen (B) from the left main bronchi showed granulomatous inflammation with caseating necrosis (H&E stain, ×100).
Reference
-
1. Aletaha D, Smolen JS. The rheumatoid arthritis patient in the clinic: comparing more than 1,300 consecutive DMARD courses. Rheumatology (Oxford). 2002; 41:1367–1374. PMID: 12468815.
Article2. Pincus T, Yazici Y, Sokka T, Aletaha D, Smolen JS. Methotrexate as the "anchor drug" for the treatment of early rheumatoid arthritis. Clin Exp Rheumatol. 2003; 21(5):Suppl 31. S179–S185. PMID: 14969073.3. Koh WJ, Kwon OJ, Jeon K, Kim TS, Lee KS, Park YK, et al. Clinical significance of nontuberculous mycobacteria isolated from respiratory specimens in Korea. Chest. 2006; 129:341–348. PMID: 16478850.
Article4. Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley C, Gordin F, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007; 175:367–416. PMID: 17277290.
Article5. Shih JY, Wang HC, Chiang IP, Yang PC, Luh KT. Endobronchial lesions in a non-AIDS patient with disseminated Mycobacterium avium-intracellulare infection. Eur Respir J. 1997; 10:497–499. PMID: 9042656.6. Mehle ME, Adamo JP, Mehta AC, Wiedemann HP, Keys T, Longworth DL. Endobronchial Mycobacterium avium-intracellulare infection in a patient with AIDS. Chest. 1989; 96:199–201. PMID: 2736976.7. Lee JH, Son KS, Park JH, Kim JC, Lee HW, Kim CH. Mycobacterium avium infection presenting as endobronchial lesions in an immunocompetent patient. Tuberc Respir Dis. 2006; 60:571–575.8. O'Brien RJ, Geiter LJ, Snider DE Jr. The epidemiology of nontuberculous mycobacterial diseases in the United States: results from a national survey. Am Rev Respir Dis. 1987; 135:1007–1014. PMID: 3579001.9. Rosenzweig SD, Holland SM. Defects in the interferon-gamma and interleukin-12 pathways. Immunol Rev. 2005; 203:38–47. PMID: 15661020.
Article10. Kolokotronis A, Avramidou E, Zaraboukas T, Mandraveli K, Alexiou S, Antoniades D. Oral tuberculosis associated with a treatment with anti-rheumatic drugs. J Oral Pathol Med. 2006; 35:123–125. PMID: 16430744.
Article11. Lee JY, Yi CA, Kim TS, Kim H, Kim J, Han J, et al. CT scan features as predictors of patient outcome after bronchial intervention in endobronchial TB. Chest. 2010; 138:380–385. PMID: 20299630.
Article12. Watanabe Y, Murakami S, Iwa T. Bronchial stricture due to endobronchial tuberculosis. Thorac Cardiovasc Surg. 1988; 36:27–32. PMID: 3376086.
Article13. Iikuni N, Kitahama M, Ohta S, Okamoto H, Kamatani N, Nishinarita M. Evaluation of Pneumocystis pneumonia infection risk factors in patients with connective tissue disease. Mod Rheumatol. 2006; 16:282–288. PMID: 17039308.14. Luis M, Pacheco-Tena C, Cazarin-Barrientos J, Lino-Perez L, Goycochea MV, Vazquez-Mellado J, et al. Comparison of two schedules for administering oral low-dose methotrexate (weekly versus every-other-week) in patients with rheumatoid arthritis in remission: a twenty-four week, single blind, randomized study. Arthritis Rheum. 1999; 42:2160–2165. PMID: 10524688.15. Visser K, Katchamart W, Loza E, Martinez-Lopez JA, Salliot C, Trudeau J, et al. Multinational evidence-based recommendations for the use of methotrexate in rheumatic disorders with a focus on rheumatoid arthritis: integrating systematic literature research and expert opinion of a broad international panel of rheumatologists in the 3E Initiative. Ann Rheum Dis. 2009; 68:1086–1093. PMID: 19033291.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Vertebral Osteomyelitis due to Mycobacterium intracellulare in an Immunocompetent Elderly Patient After Vertebroplasty
- Acute pneumonia caused by mycobacterium intracellulare
- Endobronchial Involvement of Mycobacterium intracellulare in a Patient with Previously Treated Lung Cancer
- Mycobacterium intracellulare pulmonary infection accompanied with pleural effusion
- A Case of Pulmonary Disease due to Mycobacterium avium-intracellulare complex
