Tuberc Respir Dis.
2010 Sep;69(3):163-170.
Characteristics of Pulmonary Tuberculosis in Elderly People
- Affiliations
-
- 1Department of Internal Medicine, Chungnam National University College of Medicine, Daejeon, Korea. sykim@cnu.ac.kr
Abstract
- BACKGROUND
Pulmonary tuberculosis remains a health concern in Korea despite major progress in the development of new strategies for diagnosing and treating tuberculosis. In particular, the diagnosis of newly developed pulmonary tuberculosis is on the rise in elderly persons. The aim of this study was to investigate the clinical, radiographic characteristics, and treatment outcomes of pulm onary tuberculosis in the elderly.
METHODS
The medical records of 113 young (<65 years old) and 112 elderly (> or =65 years old) pulmonary tuberculosis patients diagnosed at Chungnam National University hospital between January 2007 and December 2008 were reviewed.
RESULTS
There was no difference in the prevalence of typical symptoms between the younger and the elderly group. Dypsnea was the only symptom that occurred more frequently in the elderly group (16.8% vs 5.5%, p=0.008). On radiological study, pneumonic infiltration type was more common in the elderly group (28.6% vs 16.8%, p=0.035). Sputum Acid fast bacilli smear positivity rate was similar between the 2 groups. Elderly patients with anti-tuberculosis medication had more frequent adverse drug reactions; however, there was no significant difference between the 2 groups in the number of patients required to stop medication due to an adverse drug reaction. There were more patients lost to follow-up in the elderly group (22/112, 19.6% vs 11/113, 9.7%, p=0.036).
CONCLUSION
The majority of elderly patients did not complete the treatment, resulting in a poorer outcome. Therefore, we need to make an effort to support the continued screening of elderly patients by making this economically feasible.
Keyword
MeSH Terms
Figure
-
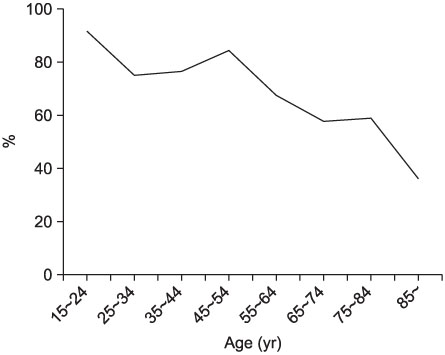
Figure 1 Age associated decrease in percentage of cure rates in pulmonary tuberculosis (p=0.033).
Reference
-
1. Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC. Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence, and deaths globally. JAMA. 2005. 293:2767–2775.2. Park JS. Treatment of pulmonary tuberculosis in elderly. Korean J Med. 2008. 75:141–148.3. Dutt AK, Stead WW. Tuberculosis in the elderly. Med Clin North Am. 1993. 77:1353–1368.4. Mackay AD, Cole RB. The problems of tuberculosis in the elderly. Q J Med. 1984. 53:497–510.5. Ryu WJ. Treatment guidelines for tuberculosis. 2005. Seoul: The Korean Academy of Tuberculosis and Respiratory Disease.6. Veen J, Raviglione M, Rieder HL, Migliori GB, Graf P, Grzemska M, et al. Standardized tuberculosis treatment outcome monitoring in Europe. Recommendations of a Working Group of the World Health Organization (WHO) and the European Region of the International Union Against Tuberculosis and Lung Disease (IUATLD) for uniform reporting by cohort analysis of treatment outcome in tuberculosis patients. Eur Respir J. 1998. 12:505–510.7. Leung CC, Yew WW, Chan CK, Chau CH, Tam CM, Lam CW, et al. Tuberculosis in older people: a retrospective and comparative study from Hong Kong. J Am Geriatr Soc. 2002. 50:1219–1226.8. Wang CS, Chen HC, Yang CJ, Wang WY, Chong IW, Hwang JJ, et al. The impact of age on the demographic, clinical, radiographic characteristics and treatment outcomes of pulmonary tuberculosis patients in Taiwan. Infection. 2008. 36:335–340.9. Katz I, Rosenthal T, Michaeli D. Undiagnosed tuberculosis in hospitalized patients. Chest. 1985. 87:770–774.10. Pérez-Guzmán C, Vargas MH, Torres-Cruz A, Villarreal-Velarde H. Does aging modify pulmonary tuberculosis? a meta-analytical review. Chest. 1999. 116:961–967.11. Rao VK, Iademarco EP, Fraser VJ, Kollef MH. The impact of comorbidity on mortality following in-hospital diagnosis of tuberculosis. Chest. 1998. 114:1244–1252.12. Patel YR, Mehta JB, Harvill L, Gateley K. Flexible bronchoscopy as a diagnostic tool in the evaluation of pulmonary tuberculosis in an elderly population. J Am Geriatr Soc. 1993. 41:629–632.13. Khan MS, Dar O, Sismanidis C, Shah K, Godfrey-Faussett P. Improvement of tuberculosis case detection and reduction of discrepancies between men and women by simple sputum-submission instructions: a pragmatic randomised controlled trial. Lancet. 2007. 369:1955–1960.14. Umeki S. Age-related changes in the manifestations of tuberculosis. Implications for drug therapy. Drugs Aging. 1991. 1:440–457.15. Davies PD. The effects of poverty and ageing on the increase in tuberculosis. Monaldi Arch Chest Dis. 1999. 54:168–171.16. Burrill J, Williams CJ, Bain G, Conder G, Hine AL, Misra RR. Tuberculosis: a radiologic review. Radiographics. 2007. 27:1255–1273.17. Kashyap S, Mohapatra PR, Saini V. Endobronchial tuberculosis. Indian J Chest Dis Allied Sci. 2003. 45:247–256.18. Kim HJ, Kim HS, Ma JE, Lee SJ, Ham HS, Cho YJ, et al. Clinical characteristics of endobronchial tuberculosis that develops in patients over 70 years of age. Tuberc Respir Dis. 2007. 63:412–416.19. Wynn GJ, Turkington PM, O'Driscoll BR. Anthracofibrosis, bronchial stenosis with overlying anthracotic mucosa: possibly a new occupational lung disorder--a series of seven cases from one UK hospital. Chest. 2008. 134:1069–1073.20. Cohen AG. Atelectasis of the right middle lobe resulting from perforation of tuberculous lymph nodes into bronchi in adults. Ann Intern Med. 1951. 35:820–835.21. Chung MP, Lee KS, Han J, Kim H, Rhee CH, Han YC, et al. Bronchial stenosis due to anthracofibrosis. Chest. 1998. 113:344–350.22. Schaberg T, Rebhan K, Lode H. Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur Respir J. 1996. 9:2026–2030.23. Yee D, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis. Am J Respir Crit Care Med. 2003. 167:1472–1477.24. Teale C, Goldman JM, Pearson SB. The association of age with the presentation and outcome of tuberculosis: a five-year survey. Age Ageing. 1993. 22:289–293.25. Sharma SK, Balamurugan A, Saha PK, Pandey RM, Mehra NK. Evaluation of clinical and immunogenetic risk factors for the development of hepatotoxicity during antituberculosis treatment. Am J Respir Crit Care Med. 2002. 166:916–919.26. Fernández-Villar A, Sopeña B, Fernández-Villar J, Vázquez-Gallardo R, Ulloa F, Leiro V, et al. The influence of risk factors on the severity of anti-tuberculosis drug-induced hepatotoxicity. Int J Tuberc Lung Dis. 2004. 8:1499–1505.27. van den Brande P, van Steenbergen W, Vervoort G, Demedts M. Aging and hepatotoxicity of isoniazid and rifampin in pulmonary tuberculosis. Am J Respir Crit Care Med. 1995. 152:1705–1708.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Tuberculosis Verrucosa Cutis with Ulcer in a Patient with Pulmonary Tuberculosis
- Treatment of pulmonary tuberculosis in elderly
- Clinical charateristics of elderly patients with plmonary tuberculosis
- Tuberculosis Verrucosa Cutis in a Patient with Pulmonary Tuberculosis
- A Study on Support by Families of Patients with pulmonary Tuberculosis and Compliance with Sick Role Behavior
