Esophageal pH and Combined Impedance-pH Monitoring in Children
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Korea. keyers@naver.com
Abstract
- Esophageal pH monitoring is considered the gold standard for the diagnosis of gastroesophageal reflux disease because of the normal ranges across the pediatric age range. However, this method can only detect acid reflux. Multichannel intraluminal impedance-pH (MII-pH) monitoring has recently been used for the detection of bolus reflux in infants and children. This method allows for the detection of liquid, gas or mixed reflux in addition to acid, weakly acidic or weakly alkaline reflux. MII-pH monitoring can record the direction of flow and the height of reflux, which are useful parameters to identify an association between symptoms and reflux. However, the technique is limited by its high cost and the lack of normative data of MII-pH in the pediatric population. Despite certain limitations, MII-pH monitoring will become more common and gradually replace pH monitoring in the future, because pH monitoring is part of MII-pH.
MeSH Terms
Figure
-
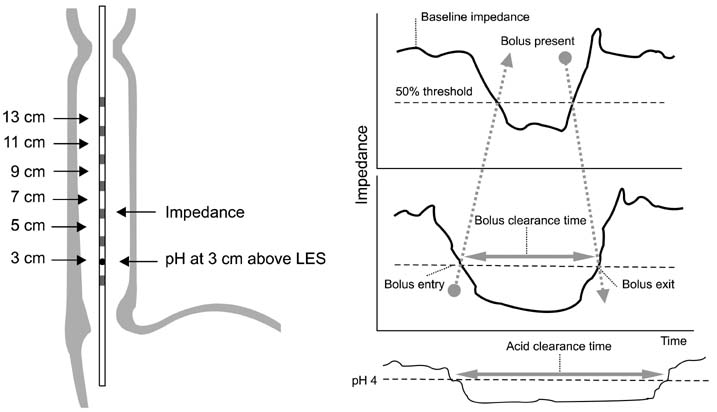
Fig. 1 Pediatric type probe and bolus acid reflux in multichannel intraluminal impedance-pH (MII-pH) monitoring. A combined MII-pH probe has 6 impedance channels and a pH sensor. The impedance electrodes are 2 cm apart from each other and the pH sensor is in the middle of the most distal impedance channel. The pH sensor is placed 3 cm above the lower esophageal sphincter (LES). The probe with the internal reference electrode crosses the LES. As the bolus reaches the impedance channel, impedance decreases rapidly. Bolus entry occurs at the 50% drop in impedance from baseline and bolus exit occurs above the 50% threshold value. Bolus reflux is defined as an impedance drop in at least 2 distal channels. Bolus clearance time is the time from bolus entry to exit. The retrograde bolus reflux is shown as bolus entry progression from distal to proximal impedance channels (dashed arrows) followed by proximal to distal bolus exit progression. Bolus reflux episodes during which the pH drops from above to below 4 are considered acid. Acid clearance time is the tie of esophageal exposure to a pH<4.
Reference
-
1. Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr. 2009; 49:498–547.
Article2. Sherman PM, Hassall E, Fagundes-Neto U, Gold BD, Kato S, Koletzko S, et al. A global, evidence-based consensus on the definition of gastroesophageal reflux disease in the pediatric population. Am J Gastroenterol. 2009; 104:1278–1295. quiz 1296.
Article3. Spencer J. Prolonged pH recording in the study of gastro-oesophageal reflux. Br J Surg. 1969; 56:912–914.4. Rudolph CD, Mazur LJ, Liptak GS, Baker RD, Boyle JT, Colletti RB, et al. North American Society for Pediatric Gastroenterology and Nutrition. Guidelines for evaluation and treatment of gastroesophageal reflux in infants and children: recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr. 2001; 32:Suppl 2. S1–S31.5. Silny J. Intraluminal multiple electric impedance procedure for measurement of gastrointestinal motility. Neurogastroenterol Motil. 1991; 3:151–162.
Article6. Lee SH, Jang JY, Yoon IJ, Kim KM. Usefulness of multichannel intraluminal impedance-pH metry in children with suspected gastroesophageal reflux disease. Korean J Gastroenterol. 2008; 52:9–15.7. Shin MS, Shim JO, Moon JS, Kim HS, Ko JS, Choi JH, et al. Impedance-pH monitoring and conventional pH monitoring are complementary methods to detect association between gastroesophageal reflux and apnea-related symptoms in preterm infants and neonates. J Matern Fetal Neonatal Med. 2012; 25:2406–2410.
Article8. Wenzl TG, Benninga MA, Loots CM, Salvatore S, Vandenplas Y. ESPGHAN EURO-PIG Working Group. Indications, methodology, and interpretation of combined esophageal impedance-pH monitoring in children: ESPGHAN EURO-PIG standard protocol. J Pediatr Gastroenterol Nutr. 2012; 55:230–234.
Article9. Working Group of the European Society of Pediatric Gastroenterology and Nutrition. A standardized protocol for the methodology of esophageal pH monitoring and interpretation of the data for the diagnosis of gastroesophageal reflux. J Pediatr Gastroenterol Nutr. 1992; 14:467–471.10. Vandenplas Y. Challenges in the diagnosis of gastroesophageal reflux disease in infants and children. Expert Opin Med Diagn. 2013; 7:289–298.
Article11. Tutuian R, Castell DO. Review article: complete gastro-oesophageal reflux monitoring - combined pH and impedance. Aliment Pharmacol Ther. 2006; 24:Suppl 2. 27–37.
Article12. van Wijk MP, Benninga MA, Omari TI. Role of the multichannel intraluminal impedance technique in infants and children. J Pediatr Gastroenterol Nutr. 2009; 48:2–12.
Article13. Wenzl TG, Schenke S, Peschgens T, Silny J, Heimann G, Skopnik H. Association of apnea and nonacid gastroesophageal reflux in infants: Investigations with the intraluminal impedance technique. Pediatr Pulmonol. 2001; 31:144–149.
Article14. Rosen R, Nurko S. The importance of multichannel intraluminal impedance in the evaluation of children with persistent respiratory symptoms. Am J Gastroenterol. 2004; 99:2452–2458.
Article15. Mousa H, Woodley FW, Metheney M, Hayes J. Testing the association between gastroesophageal reflux and apnea in infants. J Pediatr Gastroenterol Nutr. 2005; 41:169–177.
Article16. Magistà AM, Indrio F, Baldassarre M, Bucci N, Menolascina A, Mautone A, et al. Multichannel intraluminal impedance to detect relationship between gastroesophageal reflux and apnoea of prematurity. Dig Liver Dis. 2007; 39:216–221.
Article17. Loots CM, Benninga MA, Davidson GP, Omari TI. Addition of pH-impedance monitoring to standard pH monitoring increases the yield of symptom association analysis in infants and children with gastroesophageal reflux. J Pediatr. 2009; 154:248–252.
Article18. Colletti RB, Christie DL, Orenstein SR. Statement of the North American Society for Pediatric Gastroenterology and Nutrition (NASPGN). Indications for pediatric esophageal pH monitoring. J Pediatr Gastroenterol Nutr. 1995; 21:253–262.
Article19. Peter CS, Wiechers C, Bohnhorst B, Silny J, Poets CF. Influence of nasogastric tubes on gastroesophageal reflux in preterm infants: a multiple intraluminal impedance study. J Pediatr. 2002; 141:277–279.
Article20. Strobel CT, Byrne WJ, Ament ME, Euler AR. Correlation of esophageal lengths in children with height: application to the Tuttle test without prior esophageal manometry. J Pediatr. 1979; 94:81–84.
Article21. Mousa HM, Rosen R, Woodley FW, Orsi M, Armas D, Faure C, et al. Esophageal impedance monitoring for gastroesophageal reflux. J Pediatr Gastroenterol Nutr. 2011; 52:129–139.
Article22. Mainie I, Tutuian R, Shay S, Vela M, Zhang X, Sifrim D, et al. Acid and non-acid reflux in patients with persistent symptoms despite acid suppressive therapy: a multicentre study using combined ambulatory impedance-pH monitoring. Gut. 2006; 55:1398–1402.
Article23. Loots CM, van Wijk MP, Blondeau K, Dalby K, Peeters L, Rosen R, et al. Interobserver and intraobserver variability in pH-impedance analysis between 10 experts and automated analysis. J Pediatr. 2012; 160:441–446.
Article24. López-Alonso M, Moya MJ, Cabo JA, Ribas J, del Carmen Macías M, Silny J, et al. Twenty-four-hour esophageal impedance-pH monitoring in healthy preterm neonates: rate and characteristics of acid, weakly acidic, and weakly alkaline gastroesophageal reflux. Pediatrics. 2006; 118:e299–e308.25. Shay S, Tutuian R, Sifrim D, Vela M, Wise J, Balaji N, et al. Twenty-four hour ambulatory simultaneous impedance and pH monitoring: a multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol. 2004; 99:1037–1043.
Article26. Zerbib F, des Varannes SB, Roman S, Pouderoux P, Artigue F, Chaput U, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedancepH monitoring in a Belgian-French cohort of healthy subjects. Aliment Pharmacol Ther. 2005; 22:1011–1021.
Article27. Breumelhof R, Smout AJ. The symptom sensitivity index: a valuable additional parameter in 24-hour esophageal pH recording. Am J Gastroenterol. 1991; 86:160–164.28. Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology. 1994; 107:1741–1745.
Article29. Rosen R, Lord C, Nurko S. The sensitivity of multichannel intraluminal impedance and the pH probe in the evaluation of gastroesophageal reflux in children. Clin Gastroenterol Hepatol. 2006; 4:167–172.
Article30. Woodley FW, Mousa H. Acid gastroesophageal reflux reports in infants: a comparison of esophageal pH monitoring and multichannel intraluminal impedance measurements. Dig Dis Sci. 2006; 51:1910–1916.
Article31. Skopnik H, Silny J, Heiber O, Schulz J, Rau G, Heimann G. Gastroesophageal reflux in infants: evaluation of a new intraluminal impedance technique. J Pediatr Gastroenterol Nutr. 1996; 23:591–598.
Article32. Condino AA, Sondheimer J, Pan Z, Gralla J, Perry D, O'Connor JA. Evaluation of infantile acid and nonacid gastroesophageal reflux using combined pH monitoring and impedance measurement. J Pediatr Gastroenterol Nutr. 2006; 42:16–21.
Article33. Peter CS, Wiechers C, Bohnhorst B, Silny J, Poets CF. Detection of small bolus volumes using multiple intraluminal impedance in preterm infants. J Pediatr Gastroenterol Nutr. 2003; 36:381–384.
Article34. Wise JL, Murray JA. Utilising multichannel intraluminal impedance for diagnosing GERD: a review. Dis Esophagus. 2007; 20:83–88.
Article35. Di Fiore JM, Arko M, Churbock K, Hibbs AM, Martin RJ. Technical limitations in detection of gastroesophageal reflux in neonates. J Pediatr Gastroenterol Nutr. 2009; 49:177–182.
Article36. Woodley FW, Mousa H. "pH-Only" acid reflux events in infants during later phases of the feeding cycle are less acidic and cleared more efficiently than classic 2-phase acid reflux events. J Pediatr Gastroenterol Nutr. 2009; 48:41–47.
Article37. Vandenplas Y, Salvatore S, Vieira MC, Hauser B. Will esophageal impedance replace pH monitoring? Pediatrics. 2007; 119:118–122.
Article38. Corvaglia L, Mariani E, Aceti A, Capretti MG, Ancora G, Faldella G. Combined oesophageal impedance-pH monitoring in preterm newborn: comparison of two options for layout analysis. Neurogastroenterol Motil. 2009; 21:1027–e81.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- How to Interpret Ambulatory 24 hr Esophageal pH Monitoring
- How to Interpret Esophageal Impedance pH Monitoring
- Achalasia Previously Diagnosed as Gastroesophageal Reflux Disease by Relying on Esophageal Impedance-pH Monitoring: Use of High-Resolution Esophageal Manometry in Children
- Yield of Combined Impedance-pH Monitoring for Refractory Reflux Symptoms in Clinical Practice
- A Review of Diagnosis of GERD
