Pediatr Gastroenterol Hepatol Nutr.
2013 Jun;16(2):89-94.
Increase in Aminotransferase Levels during Urinary Tract Infections in Children
- Affiliations
-
- 1Department of Pediatrics, Konyang University College of Medicine, Daejeon, Korea. jmyoon@kyuh.ac.kr
Abstract
- PURPOSE
The aim of this study was to evaluate the prevalence of increased aminotransferase levels and to identify associated factors in children admitted to hospital with urinary tract infections (UTIs).
METHODS
The study included children with a diagnosis of UTI who were admitted to the Konyang University Hospital from January 2007 to May 2011. The total number of patients was 249 and the mean age was 15.88+/-28.21 months. UTI was defined as a positive urine culture (>105/colony forming unit [CFU]) with pyrexia. Patients were treated by intravenous antibiotics, such as ampicillin/sulbactam, aminoglycoside, cephalosporins or vancomycin. Patients with neonatal jaundice or other liver disease were excluded. We investigated the relationship of aminotransferase levels with the type of antibiotic, degree of vesicoureteral reflux (VUR), and causative organisms.
RESULTS
Children with increased aminotransferase levels were younger than those with normal levels (p=0.001), but white blood cell count, platelet count, causative organisms, type of antibiotics and presence of VUR were not associated with aminotransferase levels. Aminotransferase levels became normal within 1 month after discharge without special measures, except in 1 case.
CONCLUSION
We found that many children with UTI have abnormal aminotransferase levels. In most cases, this change is mild and self-limiting. We conclude that increased aminotransferase level increase during UTI do not require unnecessary tests and excessive treatment.
MeSH Terms
Figure
-
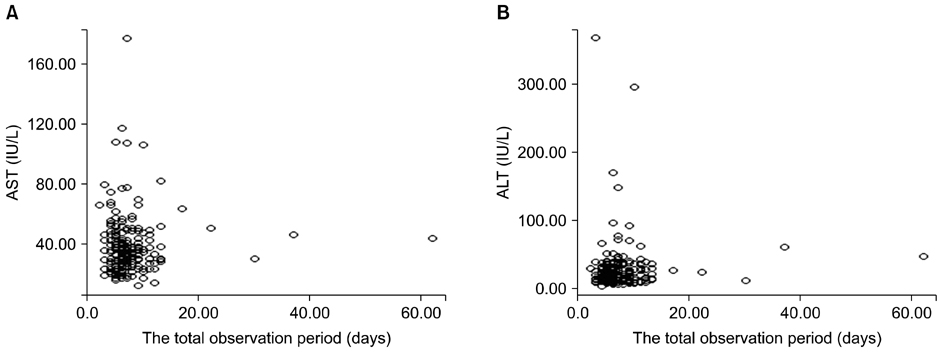
Fig. 1 Aminotransferase levels for total observation period. (A) Serum aspartate aminotransferase (AST) level and (B) serum alanine aminotransferase (ALT) level for follow up period. The follow-up period was about two months. The aminotransferase levels became normal ranges for 2 months.
Reference
-
1. Pastor CM, Billiar TR, Losser MR, Payen DM. Liver injury during sepsis. J Crit Care. 1995; 10:183–197.
Article2. Szabo G, Romics L Jr, Frendl G. Liver in sepsis and systemic inflammatory response syndrome. Clin Liver Dis. 2002; 6:1045–1066.
Article3. Van Oosten M, Rensen PC, Van Amersfoort ES, Van Eck M, Van Dam AM, Breve JJ, et al. Apolipoprotein E protects against bacterial lipopolysaccharide-induced lethality. A new therapeutic approach to treat gram-negative sepsis. J Biol Chem. 2001; 276:8820–8824.
Article4. Naito M, Hasegawa G, Ebe Y, Yamamoto T. Differentiation and function of Kupffer cells. Med Electron Microsc. 2004; 37:16–28.
Article5. Klatskin G. Hepatitis associated with systemic infections. In : Zakim D, Boyer TD, editors. Hepatology: a textbook of liver disease. Philadelphia: WB Saunders;1982. p. 711–713.6. Burkitt HG, Young B, Heath JW. Wheater's functional histology: a text and colour atlas. 3rd ed. Edinburgh: Churchill Livingstone;1993.7. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ. 2005; 172:367–379.
Article8. Dahn MS, Lange P, Lobdell K, Hans B, Jacobs LA, Mitchell RA. Splanchnic and total body oxygen consumption differences in septic and injured patients. Surgery. 1987; 101:69–80.9. Dhainaut JF, Marin N, Mignon A, Vinsonneau C. Hepatic response to sepsis: interaction between coagulation and inflammatory processes. Crit Care Med. 2001; 29:7 Suppl. S42–S47.
Article10. Marshall JC. Inflammation, coagulopathy, and the pathogenesis of multiple organ dysfunction syndrome. Crit Care Med. 2001; 29:7 Suppl. S99–S106.
Article11. Chand N, Sanyal AJ. Sepsis-induced cholestasis. Hepatology. 2007; 45:230–241.
Article12. Vermillion SE, Gregg JA, Baggenstoss AH, Bartholomew LG. Jaundice associated with bacteremia. Arch Intern Med. 1969; 124:611–618.
Article13. Moseley RH. Sepsis and cholestasis. Clin Liver Dis. 1999; 3:465–475.
Article14. Neale G, Caughey DE, Mollin DL, Booth CC. Effects of intrahepatic and extrahepatic infection on liver function. Br Med J. 1966; 1:382–387.
Article15. Campos J, Alende R, Gonzalez-Quintela A. Abnormalities in aminotransferase levels during acute pyelonephritis. Eur J Intern Med. 2009; 20:e53–e56.
Article16. File TM Jr, Tan JS, Salstrom SJ. Clinical evaluation of ceftriaxone. Clin Ther. 1984; 6:653–661.
